알레르기 비염의 백문 백답, One hundred Qs & As on allergy rhinitis
Q.
알레르기 비염은 유전병입니까
A.
그렇습니다.
대를 이어 체염색체 우성으로 유전됩니다.
이 병은 한집안의 할아버지, 아버지, 아들딸 모두에게 유발될 수 있습니다.
Q.
알레르기 비염은 흔한 병입니까.
A.
- 미국 전 연령층 사람들의 15∼22%가 알레르기 비염으로 고생하고 있습니다.
- 또 다른 연구에 의하면, 8.8~16%의 미국 사람들이 알레르기 비염으로 고생하고 있습니다.
- 다른 연구에 의하면, 20~30%의 소아청소년들이 알레르기 비염으로 고생하고 있습니다.
- 그 발병률은 증가 추세에 있습니다.
- 사춘기 이전 미국 소아들의 10%,
- 미국 사춘기 아이들과 젊은이들의 20%가 알레르기 비염을 앓고 있습니다.
- 13,579명의 미국 0-17세 연령층 소아청소년들을 대상으로 조사한 결과에 의하면, 알레르기 비염의 발병률은 0~4세 연령층에서 4.8%,
- 5~11세 연령층에서 10.5%,
- 12~17세 연령층에서 14.2% 이었습니다.
- 소아청소년들 100명 중 약 10~20명이 알레르기 비염을 앓고 있다고 생각할 수 있습니다.
- 호흡계의 만성 질환 중 가장 흔한 질환이 알레르기 비염입니다.
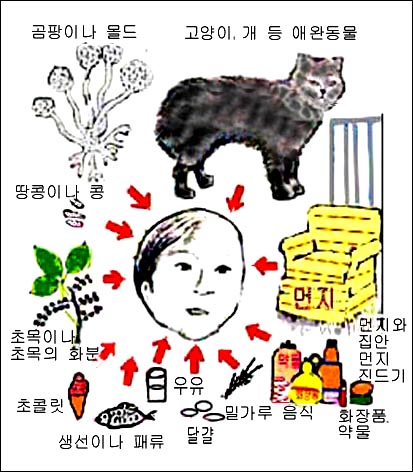
그림 3. 알레르기 질환을 유발시킬 수 있는 항원
- 개, 고양이 등 애완동물의 털, 비듬, 집 먼지 진드기(집 먼지 좀 진드기),곰팡이,몰드,화분,약물,생선이나 어패류,우유와 우유 음식물,달걀,밀가루 음식물화장품,초콜릿,견과류,땅콩,콩 등
- 알레르기를 비교적 더 흔히 유발시킬 수 있는 항원들이다.
- 심한 알레르기 비염이 있는 아이들에게 아데노이드 얼굴형(알레르기 안모)이 생길 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Q.
알레르기 비염의 원인과 발병기전은?
A.
이미 말씀드린 바와 같이 알레르기 비염에 걸릴 수 있는 체염색체 우성으로 유전되는 유전인자를 소지하고 태어납니다.
거기다가 알레르기를 일으킬 수 있는 항원이 코를 통해서, 경구, 위장관 점막층을 통해서, 피부나 점막층을 통해서, 신체의 다른 계통의 다른 기관을 통해서 신체 내로 들어와서 항원 항체 이상작용이 비강 점막층에서 생깁니다.
그때 비만세포에서 히스타민 과립체가 방출되고 그 외 다른 생화학 물질이 복합적으로 작용해서 알레르기 비염이 유발됩니다.
Q.
알레르기 비염을 일으키는 항원 역할을 하는 것들은 어떤 것이 있나요?
A.
- 숨 쉴 때 비강을 통해서 기도 속으로 흡입된 초목의 꽃가루, 곰팡이, 몰드, 개, 고양이, 소, 말, 닭, 새 등의 털이나 비듬, 깃털, 침, 죽은 곤충 가루, 집 먼지 좀 진드기, 집 먼지 등이 알레르기 비염을 유발시킬 수 있습니다.
- 경구와 위장관을 통해 섭취된 우유, 달걀, 초콜릿, 밀가루 음식, 콩, 생선, 땅콩 등의 항원이 피 속으로 들어간 후 비강의 점막층에 도달해서 알레르기 비염을 일으킬 수 있습니다.
- 피부나 각 기관의 점막층 등을 통해 신체 내로 들어온 항원이 알레르기 비염을 일으킬 수 있습니다.
- 고양이의 털, 비듬, 또는 침 등이 비강 속으로 직접 흡입될 때 알레르기 비염이 비강 내 점막층에 생길 수 있습니다.

사진 5. 사진에서 보는 음식물로 인해 각종 알레르기 질환이 유발되기 쉽다. 우유, 우유 음식물, 생선, 밀, 조개 등 어패류, 달걀, 땅콩, 호두 등 견과류 등의 음식물은 비교적 더 흔히 알레르기를 유발시킬 수 있다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
- 비강 점막층이 고양이 털이나 비듬, 또는 침에 더 이상 접촉되지 않으면 고양이의 털, 비듬, 또는 침 등으로 알레르기 비염이 더 이상 생기지 않는 것이 보통이다.
- 비강 점막층이 고양이의 털, 침, 비듬 등에 또다시 접촉될 때 고양이 털 항원으로 알레르기 비염이 다시 생길 수 있다.
Q.
알레르기 비염이 유발되는 기전은?
A.
알레르기 비염을 유발시킬 수 있는 항원이 비강 점막층에 도착하면 비만세포에서 히스타민 과립체가 방출되어 비강 점막층이 붓고, 비강의 모세혈관이 충혈 되고, 콧물이 나고, 코가 가렵고, 눈이 붉어지고 가렵고, 코가 막히고, 입을 벌리고 숨을 쉬는 증상 징후가 생기는 것이 보통이다.
알레르기 비염이 장기간 지속되면 알레르기 설루트, 알레르기 샤이나, 부정교합 등의 증상 징후가 생길 수 있다.
심하면 아데노이드 안모도 생길 수 있다.
Q.
미국에서 알레르기 비염을 치료하는 데 드는 연간 의료비가 어느 정도인가?
A
연간 4억 5천만 불의 진료비가 소요된다고 합니다.
Q.
만성 알레르기 비염이 있는 아이들에게 나타날 수 있는 증상 징후에는 어떤 것이 있는가요.
A.
- 이상 설명한 여러 가지 주 증상 징후 이외 때로는
- 수면장애,
- 학습 장애,
- 집중력 결여증(주의력 결핍 장애) 및, 또는 행동과다증(과다활동장애),
- 아데노이드 비대,
- 편도비대,
- 앞 목 부위 림프절 비대,
- 아데노이드 안모,
- 폐쇄성 수면 무호흡증(수면차단 무호흡증),
- 이갈기, 부정교합,
- 다 체모증,
- 손바닥 과다 잔금,
- 알레르기 설루트 (Allergic salute),
- 콧등 횡선(Dennie’s lines),
- 코 폴립 등의 증상 징후가 생길 수 있습니다.
Q.
알레르기 비염을 앓는 아이들에게 더 잘 생길 수 있는 다른 병도 있나요.
A
부비동염과 기관지 천식, 눈 알레르기, 중이염, 결막염 등이 동시에 생기기도 합니다.
Q.
아토피 체질이란 무엇입니까?
A.
전형적인 정상 체질이 아닌 체질을 아토피 체질 또는 아토피라고 합니다.
요즘 아토피 체질이 아닌 사람은 거의 없는 것 같습니다.
아토피 체질을 가진 아이들은 알레르기 비염, 기관지 천식(천식), 아토피 피부염, 옻 접촉성 피부염, 두드러기 등 알레르기 질환에 더 잘 걸리고 아토피 체질인 아이들에게는 식품 알레르기도 더 잘 생깁니다.
Q.
알레르기 비염과 기관지 천식은 어떤 관련이 있는가요.
A.
- 기관지 천식(천식)이 있던 과거 병력이 있는 아이들의 90%에게 알레르기 비염이 유발될 수 있고, 알레르기 비염이 잘 치료되면 기관지 천식도 잘 치료될 수 있습니다.
- 알레르기 비염을 앓는 환아들에게 기관지 천식이 생기는 빈도는 알레르기 비염이 없는 아이들에게 기관지 천식이 생기는 빈도보다 3배 이상 더 높다.
- 알레르기 비염을 앓는 환아들은 기관지 천식을 앓을 확률이 40%라고 한다.
- 알레르기 비염과 기관지 천식은 IgE, 사이토카인, 히스타민, 류코트리엔 등 생화학 매개로 인해서 유발되고 기관지 천식은 코르티코스테로이드제, 기관지확장제, 항류코트엔제, 항 IgE제 등으로 치료될 수 있으며 알레르기 비염은 기관지 천식을 치료하는데 쓰는 약물 성분이 든 알레르기 비염 약물로 잘 치료될 수 있습니다.
Q.
계절적 알레르기 비염, 통년성 알레르기 비염, 혼합형 알레르기 비염이란 무엇인가?
A.
- 곰팡이나 몰드 등의 항원으로 유발된 알레르기 비염이 있는 아이들이 곰팡이나 몰드가 자라지 않는 건조한 장소에 가면 곰팡이나 몰드 항원으로 알레르기 비염이 더 이상 유발되지 않는 것이 보통입니다.
- 그 아이들이 곰팡이나 몰드가 자라는 습한 장소에 다시 가면 곰팡이나 몰드 항원으로 알레르기 비염이 또다시 유발되는 것이 보통입니다.
- 곰팡이나 몰드로 유발되는 알레르기 비염의 증상 징후는 여름철과 같이 곰팡이나 몰드가 자라기 좋은 기온이나 계절에서 더 심해질 수 있습니다.
- 또 아카시아 화분으로 알레르기 비염이 유발되어 알레르기 비염으로 고생하는 아이들은 아카시아 꽃이 만발하는 5~6월에 아카시아 꽃 화분으로 알레르기 비염이 해마다 유발될 수 있습니다.
- 이와 같이 계절에 따라 유발되는 알레르기 비염을 계절적 알레르기 비염이라고 합니다.
- 레그위드(Ragweed)가 자라는 가을철에는 레그위드 꽃가루 항원에 의해서 유발되는 알레르기 비염이 유발될 수 있고, 미 뉴잉글랜드 지방에서는 봄에 많이 피는 메이풀 트리 꽃가루 항원으로 봄철에 알레르기 비염이 많이 유발됩니다.
- 이런 종류의 알레르기 비염을 통틀어 계절적 알레르기 비염이라고 합니다.
- 거의 매일 접촉되는 집 먼지, 집 먼지 좀 진드기나, 몰드, 또는 곰팡이, 또는 거의 매일 먹는 음식물 등 항원으로 알레르기 비염이 가장 많이 유발될 수 있습니다.
- 그런 종류의 항원에 일 년 내내 접촉되는 아이들에게 알레르기 비염이 일 년 내내 유발 될 수 있습니다.
- 이런 종류의 알레르기 비염을 통년성 알레르기 비염이라 합니다. 집 먼지 좀 진드기로 인해 유발되는 통년성 알레르기 비염(일 년 내내 증상이 있는 알레르기 비염 )은 9세 이전 아이들에게는 잘 발생되지 않습니다.
- 많은 아이들에게 계절적 알레르기 비염도 생기고 통년성 알레르기 비염이 함께 있습니다.
- 이러한 알레르기 비염을 혼합형 알레르기 비염이라고 합니다.
Q.
감기나 스트레스와 알레르기 비염의 증상 징후에 서로 어떤 관계가 있나요.
A.
일반적으로, 감기나 독감 등 바이러스성 상기도 감염병에 걸리거나 스트레스를 많이 받을 때는 알레르기 비염의 증상 징후가 훨씬 더 심해질 수 있습니다.
또 더 많은 종류의 항원에 더 많이 노출될 때 그 증상 징후가 더 심해질 수 있습니다.
Q.
급성 알레르기 비염의 전형적 증상징후는 무엇인가요.
A.
- 나이, 항원의 종류, 합병증의 유무 등에 따라 다릅니다.
- 알레르기 비염의 전형적인 증상은 다음과 같습니다.
- 콧물이 나고
- 코가 막히고, 가렵고
- 재채기하고
- 눈이 붉고, 가렵고, 눈물이 날 수 있고
- 입천장이 가려울 수 있고
- 이런 증상 징후가 계절에 따라 재발될 수 있고
- 이런 증상 징후가 일시적으로 유발될 수 있으며 한 계절 내내 유발될 수 있습니다.
- 그런 증상 징후가 경도로, 중등도로, 또는 중증으로 나타날 수 있습니다.
Q.
신생아나 영아에게도 알레르기 비염은 생길 수 있나요.
A.
이론적으로, 알레르기 비염의 증상 징후는 신생아기부터 시작될 수 있고 그 후 어느 연령층에서도 시작될 수 있습니다.
우유 단백질이 든 인공영양을 먹기 시작하면, 특히 아토피 체질을 가진 신생아에게 알레르기 비염이 유발되기 시작합니다.
모유를 먹는 아기에게 알레르기 비염이 덜 생길 수 있지만, 수유모가 먹은 음식물에 따라 알레르기 비염이 신생아에게도 생길 수 있고 영유아에게도 유발될 수 있습니다.
Q.
우유나 우유 음식물로 유발될 수 있는 알레르기 비염의 발생률은 얼마나 되나요.
A.
우유나 우유로 만든 음식물로 유발되는 알레르기 비염의 발병률은 0.3% 정도입니다.
Q.
아토피 체질이 있는 신생아들과 영아들이 먹는 인공영양과 알레르기 비염과 어떤 관련이 있나요.
A.
신생아나 영아, 특히 아토피 체질이 있는 신생아와 영아가 우유 단백질이 든 인공영양, 전우유(전유/Whole milk), 우유 음식물을 먹으면 우유 단백질로 알레르기 비염이 유발될 수 있습니다.
Q.
여러 가지 항원들에 한꺼번에 노출되면 알레르기 비염이 더 심해질 수 있는가요.
A.
우유 음식물에 알레르기 비염이 있는 아이들이 집 먼지 좀 진드기에 노출될 때 집집 먼지 좀 진드기 항원으로 알레르기 비염이 유발될 가능성이 더 있고, 또 우유 단백질로 인한 알레르기 비염과 집 먼지 좀 진드기로 인한 알레르기 비염이 동시에 유발될 수 있습니다.
Q.
‘알레르기 설루트’란 말은?
A.
알레르기 비염으로 코가 가려우면 코를 문지르기 위해 손을 들어 마치 경례하는 자세로 코를 손으로 문지르는 증상 징후가 있습니다.
이런 증후를 ‘알레르기 설루트’(Allergy salute)라고 합니다.
Q.
알레르기 비염과 구강호흡과는 무슨 관계가 있나요.
A.
- 알레르기 비염으로 코가 막히면 입을 벌리고 입으로 숨을 쉴 때가 많습니다.
- 이런 호흡을 ‘구강호흡’이라 하고 ‘게이핑’(Gaping)이라고도 합니다.
- 만성 알레르기 비염이 있으면 밤낮을 가리지 않고 아무 사람들 앞에서 입을 벌리고 숨을 쉬는 경향이 많습니다.
- 때로는 그렇게 고생하는 아이들을 보고 ‘바보’라고 말하는 바보 같은 어른들도 있습니다.
- 신생아들이나 영아들에게 알레르기 비염이 생기면 코가 자주 막혀 입을 벌리고 숨 쉴 때가 잦습니다.
- 이런 증상을 영어로 게이핑(Gaping)이라 하고 한글로 ‘구강호흡’이라 합니다.
- 알레르기 비염이 적절히 잘 치료되지 않으면 이런 증상 징후가 신생아기 때부터 사춘기까지 계속될 수 있고 성인이 된 후에도 계속 나타날 수 있습니다.
Q.
부정교합과 알레르기 비염과의 관계는?
A
알레르기 비염이 장기간 계속되면서 구강호흡을 하고, 아데노이드가 커지고, 편도도 커지고, 입안, 얼굴의 구조 상호관계의 변화가 생기고 치열에도 문제가 생길 수 있습니다.
그리고 심한 부정교합이 생길 수 있습니다.
여기에도 찬반론이 있습니다.
저의 경험으로 보면 부정교합과 알레르기 비염과는 밀접한 관계가 있습니다.
그래서 알레르기 비염 치료는 부정교합 치료에 중요한 역할을 한다고 생각합니다.
Q.
알레르기 비염과 아데노이드 안모는 어떤 관계가 있나요?
A
알레르기 비염으로 입을 벌리고 숨 쉬는 증상 징후가 장기간 생길 수 있습니다.
뻐드렁니, 옥니, 부정교합 등 치열에 이상이 생길 수 있습니다. 눈, 코, 입, 얼굴, 잇몸 등의 해부학적 얼굴 구조의 상호관계 변화가 생기고 이상이 생길 수 있습니다.
그래서 특이한 안모의 상이 알레르기 비염이 있는 아이에게 나타날 수 있습니다.
이런 안모를 아데노이드 안모라고 합니다.
Q.
감기와 알레르기 비염은 어떤 차이가 있나요.
A.
- 감기는 코, 비강, 인두, 부비동, 아데노이드, 편도 등 상기도 기도 부분에 생기는 바이러스성 감염병입니다.
- 감기에 걸리면 미열이나 고열이 나고 인두가 아프고 몸이 아픈 것이 보통입니다.
- 그 감기는 대개 10일 이내 자연히 낫습니다.
- 알레르기 비염에 걸리면 비강 내 점막층이 붓고, 충혈 되고, 코가 막히고, 콧물이 나고, 재채기를 할 수 있으며 코가 막히면 코로 숨을 잘 쉴 수 없으므로 입을 벌리고 입으로 숨을 쉴 수 있습니다.
- 잠도 잘 자지 못합니다.
- 알레르기 비염은 알레르기성 질환이고 알레르기 비염을 앓을 때는 열이 나지 않고 인두통도 없고 몸이 아프지도 않고 2주 이상 계속되는 것이 보통입니다.
- 이렇게 감기와 알레르기 비염은 다릅니다.
- 때로는 이 두 병이 함께 있을 수 있습니다.
Q.
알레르기 비염과 아데노이드 또는 편도와의 관계에 어떤 것이 있나요.
A.
- 아데노이드는 비강의 맨 뒤 부위, 인두의 맨 위 부위에 위치한 일종의 림프조직입니다.
- 아데노이드는 코를 통해서 들어오는 황원, 세균, 바이러스 등을 잡아 상기도 이외 신체내 더 깊숙이 들어가지 못하게 하는 감염병 방어기능을 합니다.
- 콧속을 통해 몸속으로 들어오는 해로운 항원을 잡아 체내로 더 이상 들어오지 못하게 하는 일도 합니다.
- 이런 기능을 과도하게 하면 결과적으로 아데노이드가 해부학적으로 비대해 집니다.
- 거의 같은 이치로 입안 양쪽에 있는 구개 편도도 커지게 됩니다.
- 특히 알레르기 비염이 있는 아이들의 아데노이드와 편도는 비정상적으로 더 많이 커져 있는 것이 보통입니다.
Q.
알레르기 비염이 있는 아이들이 코 먹은 소리도 하고 코를 더 자주 곤다는데, 이유는 무엇입니까
A.
알레르기 비염이 있는 아이들의 아데노이드와 편도가 비정상적으로 더 커지고 코가 막혀 구강호흡을 하고 비강, 구개, 치열 등 해부학적 구조에 변화가 생깁니다.
그로 인해서 말을 할 때 코 먹은 소리를 내고 잠잘 때 코를 고는 경우가 많습니다.
특히 학령기 아이들에게 알레르기 비염이 있으면 코가 자주 막힐 수 있고 비강의 후부에 있는 아데노이드와 입안 양쪽에 있는 편도가 비정상적으로 많이 커질 수 있습니다.
그런 이유로도 코를 더 잘 곱니다.
Q.
알레르기 비염이 있으면 코피가 잘 난다고 하는데. 왜 그런가요?
A.
알레르기 비염이 있으면 비강 점막층이 붓고, 창백하고, 습하고, 그 점막층에 있는 모세혈관이 확장됩니다.
재채기를 하든지 기침, 사소한 코 외상, 또는 코를 살짝 문지르거나 코를 자칫 건드리기만 해도 확장된 점막층 모세혈관이 터져 코피가 더 잘 날 수 있습니다.
Q.
알레르기 비염이 있어도 기침을 하나요?
A.
- 알레르기 비염이 있으면 기침을 간간이 조금 할 수 있습니다. 특히, 밤에 누워 잘 때 콧물이 비강의 후부, 비인두 부위로 흘러가서 그로 인해 인두가 자극받아 자다가 기침을 간간이 할 수 있습니다.
- 또 알레르기 비염이 있는 아이들의 30%는 기관지 천식을 동시에 앓고 있습니다.
- 그 때문에도 기침을 할 수 있고 때로는 알레르기 비염과 기관지 천식 이 두 병으로 기침을 할 수 있습니다.
- 기관지 천식이 있는 아이들의 대부분은 밤에 자는 동안 야간성 기관지 천식 발작이 유발돼서 자다가 기침을 하는 것이 보통입니다.
- 이런 기침을 여러 날 동안 하는 경우도 있습니다.
- 이렇게 잘 때 유발되는 기관지 천식 발작을 야간성 기관지 천식이라고 합니다.
- 알레르기 비염이 있는 아이들이 밤에 자다가 기침을 할 때, 야간성 기관지 천식으로 기침을 하는지, 알레르기 비염으로 기침을 하는지, 또는 알레르기 비염과 야간성 기관지 천식, 이 두 병으로 인해서 기침을 하는지 감별 진단하기가 어려울 때도 있습니다.
Q.
알레르기 비염이 있으면 축농증(부비동염)에 잘 걸릴 수 있나요.
A.
- 그렇습니다.
- 알레르기 비염이 있으면 축농증에 더 잘 걸릴 수 있습니다.
- 비강 점막층과 부비동 점막층은 같은 종류의 점막층 세포로 형성되어 있고 부비동과 비강은 작은 자연 통기관으로 서로 연결되어 있습니다.
- 또 알레르기 비염을 일으킨 그 통기관의 점막층이 붓고 그 통로가 알레르기 비염으로 자주 막힐 수 있습니다.
- 자연 통기관이 막히면 부비동에 세균감염이 더 쉽게 생겨 축농증에 더 잘 걸립니다.
- 비강 주위에 전두동, 사골동, 접형동, 상악동 등 8개의 부비동이 얼굴 양쪽에 정상적으로 있습니다.
- 비강 속과 그 주위에 있는 부비동은 작은 통기관으로 정상적으로 서로 연결되어 있습니다.
- 그 통기관에 있는 점막층이 알레르기 비염으로 부어 통기관이 막힐 수 있고, 그로 인해 부비동염(축농증)이 생길 수 있으며 사이누스 두통도 생길 수 있습니다.
- 이런 이유로 알레르기 비염이 있는 아이들의 대부분은 부비동염에 더 잘 걸립니다.
Q.
알레르기 비염이 있으면 두통이 자주 생길 수 있나요.
A.
알레르기 비염이 있을 때 부비동과 비강 사이를 연결하는 작은 통기관이 쉽게 막히고 그로 인해 막힌 부비동성 두통(사이누스 두통/Sinus headache)이 자주 생길 수 있습니다.
또 축농증이 생겨 축농증의 증상 징후로 두통이 생길 수 있고 아토피 체질이 있는 아이들에게 긴장성 피로 증후군이 생길 수 있으며 그로 인해서도 두통이 자주 생길 수 있습니다.
Q.
알레르기 비염이 있으면 중이염에 더 잘 걸릴 수 있나요.
A.
- 더 잘 걸릴 수 있습니다.
- 알레르기 비염으로 후비공 기도 부위에 있는 구씨관 입구(이관 입구)와 이관이 부어 이관이 자주 막힐 수 있습니다.
- 이때 중이 강 속에 음압이 생길 수 있습니다.
- 중이 강 속에 삼출액이 고일 수 있고 중이염이 생길 수 있습니다.
- 또 그에 따라 중이 강 삼출액에 세균 감염이 생겨 급성 중이염이 생길 수 있습니다.
- 구씨관(이관)이 부어 이관이 자주 막힐 수 있고, 이관을 통해 중이 강과 비인두 기도 부분 속에 있는 이관 입구 사이에 공기가 유통되지 않을 수 있습니다.
- 급성 중이염, 또는 삼출성 중이염에 자주 걸릴 수 있습니다.
- 때로는 청력 장애가 생길 수 있습니다.
Q.
알레르기 비염이 있을 때 나는 콧물과 축농증이 있을 때 나는 콧물에 차이가 있는가요.
A.
합병증이 없이 알레르기 비염만 있을 때는 주로 맑은 콧물이 나오는 것이 보통입니다.
그러나 알레르기 비염과 박테리아성 부비동염이 동시에 있을 때는 콧물이 누렇거나 퍼렇고 더 짙은 콧물이 나는 것이 보통입니다. 어떤 때는 콧물에 차이가 없습니다.
Q.
알레르기 비염이 있으면 콧물이 꼭 나오나요.
A.
알레르기 비염만 있을 때도 콧물이 안 나올 수 있고 부비동염만 있을 때도 콧물이 안 나올 수 있습니다.
또는 두 가지 병이 동시에 있을 때도 맑은 콧물이 조금씩 나올 수 있고, 때로는 콧물이 조금도 나지 않을 수 있습니다.
Q.
알레르기 비염이 있으면 눈과 입에도 알레르기 질환이 생기나요?
A.
생길 가능성이 많습니다.
눈, 부비동, 아데노이드, 편도, 인두, 구강 등에 알레르기성 질환이 동시에 유발될 수 있습니다.
예를 들면, 알레르기 결막염이 잘 생길 수 있습니다.
알레르기 결막염으로 결막이 자주 충혈 되고, 눈이 빨갛고, 눈물이 자주 나고, 눈이 가려워 눈을 자주 비빌 수 있는 증상 징후가 생길 수 있습니다.
알레르기 비염으로 지도형 혀가 자주 생길 수 있습니다.
Q.
알레르기 비염이 있는 아이들의 일부는 수면 중 숨이 막혀 무호흡증이 생길 수 있고 때로는 괴롭게 숨을 쉬거나 코를 골 수 있다는 말을 들었는데, 왜 그런가요.
A.
아토피 체질이 있는 아이들의 아데노이드는 아토피 체질이 아닌 아이들의 아데노이드보다 훨씬 더 크고 비대되어 있는 것이 보통입니다.
또 편도도 마찬가지로 더 커져 있는 경우가 대부분입니다.
그 때문에 알레르기 비염이 있는 아이들의 상기도, 즉 숨통이 훨씬 더 좁아집니다.
그래서 수면 중 잠시 숨이 막혀 괴롭게 숨 쉬거나 코를 골 수 있습니다.
때로는 차단성 무호흡증(폐쇄성 수면 무호흡증)도 생길 수 있습니다.
Q.
알레르기 비염이 있는 아이들의 일부에서 아래턱 바로 밑 목에 있는 림프절이 커져 있다는 글을 읽었는데, 왜 그런가요.
A.
알레르기 비염이 있는 아이들의 아래턱 바로 밑에 있는 목 부위에 있는 림프절이 커져있는 것이 보통입니다.
아래턱 바로 밑 목 부분 림프절도, 아데노이드와 편도도 일종의 림프조직이고 그 림프조직은 항원들이나 세균이 입이나 비강을 통해 비, 인두 강을 거쳐 몸속으로 더 이상 들어가지 못하게 하는 감염병 방어기능을 합니다.
그런 방어기능을 하다 보니 편도, 목에 있는 림프절도 과다히 커집니다.
Q.
알레르기 비염이 있는 아이들의 대부분이 밤에 자다가 이를 자주 가는 버릇이 생긴다는 데요. 왜 그런가요.
A.
알레르기 비염이 있으면, 눈과 코뿐만 아니라 인두와 입천장도 가려울 수 있습니다.
자다가 인두나 입천장 등이 가려울 때 위턱과 아래턱을 놀리어 가려움증을 해결하는 방법으로 무의식적으로 이를 간다고 주장하는 의사들도 있고 저도 그렇다고 생각합니다.
알레르기 비염이 있는 아이들의 대부분이 밤에 자다가 이를 자주 가는 버릇이 있습니다.
Q.
알레르기 비염이 있으면 구강, 얼굴 등에 어떤 변화가 생길 수 있나요.
A.
코가 자주 막혀 입을 벌리고 숨을 쉬기 때문에 구강, 얼굴, 코, 턱, 치아, 잇몸 등에 해부학적 구조의 상호 관계에 많은 변화가 알레르기 비염이 있는 아이들에게 생길 수 있습니다.
그 결과로 생긴 치아 변화 중 하나가 부정교합입니다.
둘째는 아데노이드 안모입니다. 앞에서 이미 언급했습니다.
그 외 여러 가지의 변화가 얼굴에 생길 수 있습니다.
Q.
알레르기 비염이 있는 아이들에게 때로는 체모가 더 많이 난다고 하는 데, 왜 그런가요.
A.
항원이 경구, 비강, 피부나 점막층을 통해 체내로 들어옵니다. 피부를 통해 들어오는 그런 항원이 더 이상 체내로 들어오지 못하게 방지하기 위해 체모가 더 많이 나는 것입니다.
콧구멍 속 털이 더 많이 나는 것도 거의 같은 이치입니다.
Q.
알레르기 비염을 어떻게 진단하나요?
A.
현재의 병력, 과거병력, 가족병력, 증상 징후, 진찰 소견 등을 총 종합해 진단하는 것이 일반적입니다.
필요에 따라, 알레르기 유발 검사, 알레르기 피부 시험, 혈액검사 등 다른 여러 가지 방법으로 진단합니다.
Q.
알레르기 비염이 있는 아이들이 감기에 걸리면 알레르기 비염이 없는 아이들과 달리 앓나요?
A.
알레르기 비염이 있는 아이들이 감기에 걸리거나 다른 종류의 바이러스성 상기도 염에 걸리면 알레르기 비염의 증상 징후가 더 악화될 수 있습니다.
그리고 감기 등 상기도염의 증상 징후가 훨씬 더 심하게 나타날 수 있습니다.
Q.
알레르기 비염이 있으면서 흔히 생기는 합병증과 공존이환에는 어떤 것이 있나요.
A.
알레르기 비염이 있으면 아이들은 기관지 천식, 부비동염, 중이염, 아토피성 피부염, 음식물 알레르기, 약물 알레르기, 곤충 알레르기 등의 공존이환이 있을 수 있습니다.
Q.
알레르기 비염을 진단하는 데 아주 중요한 징후 증상에는 어떤 것이 있나요.
A.
- 코가 가려워서 코를 추켜올리면서 코를 문지르는 버릇으로 코의 경골과 연골이 연결되는 콧등 피부 부위에 가로로 피부 주름살이 잡힐 수 있습니다. 피부 주름살을 데니 선(Dennie lines)이라고 합니다.
- 손을 추켜올려 코를 문지르는 징후를 ‘알레르기성 경례‘ 또는 ‘알레르기성 설루트(Allergy salutes)라고 합니다.
- 두 눈 아래 눈꺼풀의 바로 밑에 있는 피부색이 거무스름한 피부색으로 변합니다.
- 알레르기성 샤이너(Allergic shiners)라고 한다.
- 알레르기성 샤이너는 일시적으로 생길 수도 있고, 한 번 생긴 후 몇 개월 동안 또는 그 이상 오랫동안 계속 갈 수도 있습니다.
- 샤이너란 말은 얼굴이나 신체 어떤 부위가 타박상을 입었을 때 타박상을 입은 그 후 피부색이 거무스름하게 일시적으로 변화된 것을 의미합니다.
- 알레르기 비염이 오랫동안 지속될 때 코, 비강 속, 입 속, 아데노이드, 편도 등의 해부학적 상호 관계가 특이하게 변화됩니다.
- 얼굴 모양이 마치 바보 얼굴 모양으로 변할 수 있다.
- 이런 얼굴 모양을 아데노이드 얼굴형, 또는 아데노이드 안모(Adenoid face)라고 합니다.
- 이상 징후는 알레르기 비염을 진단하는데 상당한 가치가 있습니다.
Q.
알레르기 비염을 어떻게 진단하나요?
A.
이미 설명하였듯이 환아의 과거 병력과 현재의 병력, 가족 병력, 증상 징후, 진찰소견 등을 종합해서 주로 진단합니다.
필요에 따라 혈액 검사, 알레르기 피부 시험, 비경 검사. 비강 내시경 등으로 비강을 검진해서 진단합니다.
전형적 알레르기 비염의 증상 징후가 있고, 결막이 충혈 되고, 비경으로 비강을 검진할 때 비강 점막이 창백하고 비정상적으로 습한 징후 등이 있으면 이 병을 진단하는데 많은 도움이 됩니다. 그 외 이관이 자주 막히고, 기침을 간간이 하고, 부비동이 있는 부위에 압박감 등의 증상이 있을 수 있습니다.
Q.
알레르기 비염을 진단하는데 가족 병력이 중요한가요?
A.
친부모, 형제자매들 중 누군가에게 기관지 천식, 알레르기성 피부염, 알레르기 비염, 약물 알레르기, 접촉성 피부염, 음식물 알레르기 등 알레르기성 질환이 있는 가족 병력이 있으면 알레르기 비염을 진단하는데 많은 도움이 됩니다.
그리고 친부모, 형제자매 중 누구든지 아토피 체질이 있으면 진단하는 데 진단하는데 많이 도움됩니다.
Q.
알레르기 비염이 음식물 항원으로 인해서도 유발될 수 있는지 어떻게 알지요?
A.
알레르기 비염은 체 염색체 우성으로 유전된다.
알레르기 비염이 음식물 항원으로 인해서도 유발될 수 있습니다.
알레르기 비염을 유발시키는음식물에는 어떤 것이 있나 알아내는 방법 중 하나가 유발 검사입니다.
또 그 음식물을 먹는 것을 피해서 진단할 수 있습니다.
Q.
유발 검사란 무엇입니까
A.
- 음식물 항원으로 유발된 알레르기 비염을 진단하는데 유발 검사로 진단하기도 합니다.
- 알레르기 비염을 유발시킨다고 의심되는 음식물을 2∼4주 동안 일체 먹지 말고 그 음식물을 2∼4주 먹지 않는 동안 알레르기 비염의 증상 징후가 좋아지는지, 다 없어지는지, 더 하는지, 변화가 없는지 조심스럽게 관찰합니다.
- 이때 알레르기 비염의 증상 징후가 확연히 호전되면 그 음식물이 알레르기 비염을 일으켰을 가능성이 많다고 생각할 수 있습니다.
- 그러나 이런 방법으로 진단을 확실히 내릴 수는 없습니다.
- 그 다음 알레르기 비염을 유발시켰다고 의심했던 음식물을 다시 먹을 때 알레르기 비염의 증상 징후가 전과 거의 같이 다시 생기면 그 음식물은 알레르기 비염을 유발시켰을 가능성이 아주 많다고 생각할 수 있습니다.
- 이런 식으로 알레르기 비염을 유발시킨 음식물(항원)을 찾아내서 알레르기성 질환을 진단하는 방법을 유발 검사(도전 검사)라고 합니다.
- 유발 검사는 아무 때나 해서도 안 되고 부모나 환자의 마음대로 해서는 절대로 안 됩니다.
- 알레르기 비염이 경미할 때도 의사의 지시에 따라서 의사가 유발 검사를 할 수 있습니다.
Q.
집 먼지나 집 먼지 좀 진드기 등 항원으로 알레르기 비염이 유발된다고 의심할 때 유발 검사(도전 검사)를 할 수 있나요.
A.
- 할 수 있지요.
- 집 먼지나 집 먼지 좀 진드기 등의 항원으로 알레르기 비염이 유발되어 있던 아이들이 집 먼지나 집 먼지 좀 진드기가 많은 집안에 있을 때는 코가 가렵고 재채기를 많이 하면서 알레르기 비염의 증상 징후가 나타날 수 있습니다.
- 이와 같이 알레르기 비염의 증상 징후가 나타날 때 집 먼지나 집 먼지 좀 진드기 항원에 알레르기 비염이 유발됐다고 의심할 수 있습니다.
- 유발 검사로 항원을 찾는 것보다 보통 피부 알레르기 시험으로 항원을 찾는 경우가 더 많습니다.
Q.
알레르기 비염을 진단하는데 쓰는 임상검사는 어떤 것이 있나요.
A.
- IgE 혈액 검사,
- 비강 점액 검사,
- 알레르기 피부 검사,
- 혈액 호산구 검사,
- 방사선 알러젠 흡수면역 측정법(RAST),
- 섬유광시 비경 검사,
- 비강내 도발 검사,
- 비강 내 공기 유통검사,
- 비강 내시경 검서
- 비강 점막층 혈류 검사 등으로 알레르기 비염을 진단할 수 있습니다.
- 일반적으로, 소아청소년과에서는 이런 임상 검사로 진단하지 않고 알레르기 비염의 증상 징후의 유무, 진찰소견 등을 종합해서 알레르기 비염을 진단하는 것이 보통입니다.
Q.
환경 컨트롤 치료와 항원 피하는 치료에 관해서 설명을 해주세요.
A.
- 알레르기를 유발시킬 수 있는 모든 항원이나 유발 인자들을 가능한 한 피하거나 제거하는 방법이
- 이상적인 치료 방법입니다.
- 구체적으로 더 설명하면 다음과 같습니다.
- 알레르기 비염이나 다른 여러 종류의 알레르기 질환을 유발시킬 수 있는 항원– 음식물을 될 수 있는 한 먹지 말아야 합니다.
- 알레르기 질환이 있거나 아토피 체질이 있는 친부모 형제자매들에게 태어난 신생아들이나 영아들에게 우유나 우유 단백질, 또는 콩 단백질이 든 인공영양을 먹이는 대신 가능한 한 모유를 수유하든지 저 알레르기성 인공영양을 먹여 알레르기 비염이 유발되지 않게 예방하고 이미 생긴 알레르기 비염을 적절히 치료합니다.
- 알레르기 비염과 다른 알레르기 질환을 예방하기 위해 알레르기 질환을 잘 유발시킬 수 있는 그 외 음식물도 될 수 있는 한 먹지 말아야 합니다.
- 특히, 우유, 달걀, 초콜릿 등 음식물은 알레르기 비염을 비롯한 다른 종류의 알레르기성 질환을 더 잘 유발시킬 수 있는 음식물로 잘 알려져 있습니다.
- 그런 음식물을 될 수 있는 대로 피합니다. 때로는 알레르기 비염을 일으키는 음식물을 갈망하는 증상도 생길 수 있으므로 주의를 요합니다.
- 개, 고양이, 새 등의 애완동물을 가능하면 집안에서 기르지 말고 접촉하지 않는 것이 좋습니다.
- 부득이, 애완동물을 집안에서 키울 때는 동물의 털, 침, 비듬, 깃털 등에 접촉되거나 흡입되지 않게 하고 개를 자주 목욕시킵니다.
- 아토피 체질이 있거나 알레르기 비염이 있는 아이들이 사는 집안에 화초나 나무 등을 될 수 있는 한 기르지 말아야 합니다.
- 곰팡이나 몰드는 지하실 등 습한 곳에서 자라므로 집안의 습도를 적절히 조절해서 곰팡이나 몰드가 자라지 않게 합니다.
- 고정해 깐 카펫에 집 먼지가 더 많이 낄 수 있고 집안 먼지 진드기가 더 잘 자랄 수 있기 때문에 거두어 자주 빨아 쓸 수 있는 카펫을 깔든지 카펫을 깔지 않는 것이 더 좋습니다.
- 커튼을 자주 빨아 써야 한다.
- 집안의 집 먼지를 깨끗이 청소하고 집 먼지 좀 진드기가 자라지 않도록 합니다.
- 알레르기 비염이나 아토피 체질이 있는 아이들이 자는 침실에는 침구 이외 다른 것을 놓아서는 안 됩니다.
- 침대 매트리스와 스프링 박스를 플라스틱 커버로 씌워 집 먼지 좀 진드기가 자라지 않도록 합니다.
- 꽃이 만발하는 봄철에는 꽃가루나 곰팡이 등이 집안으로 들어오지 않게 창문을 꼭 닫습니다.
- 화초를 가꾸거나 잔디를 깎을 때 꽃가루나 곰팡이 등이 기도 속으로 흡입될 수 있고 그로 인해 알레르기 비염이나 알레르기성 결막염, 또는 기관지 천식이 유발될 수 있습니다.
- 그런 항원접촉을 절대적으로 피하기는 어렵지만 가능한 한 접촉을 피합니다.
- 필요에 따라 마스크를 착용하고 먼지가 눈으로 들어오는 것을 막는 안경을 쓰고 잔디를 깎아야 합니다.
- 레그위드 꽃이 피는 계절에는 레그위드 잡초가 자라는 곳에 가지 않도록 합니다.
- 동물의 털, 새 깃털로 만든 옷을 입지도 말고 깃털이나 털을 넣은 베개나 이불 등을 절대로 쓰지 않도록 합니다.
- HEPA 공기 필터나 Acaricides 등으로 집 먼지 좀 진드기 등을 감소시킵니다.
- 바퀴벌레를 박멸시킵니다.
Q.
알레르기 비염 약물 치료에 대해서 알고 싶습니다.
A.
- 항히스타민제-1세대 항히스타민과 2세대 항히스타민이 있습니다.
- 항염증제 치료,
- 항원 면역 요법
- 류코트레인 수용체 길항제 (Leukotriene receptor antagonists) 치료.
- 코르티코스테로이드제 치료.
- 비만세포(마스터 세포) 안정제 치료.
- 비강 속에 직접 넣는 비강 점막 충혈완화제 치료.
- 알파 아드레날린 작동제 치료.
- 종합제 치료.
Q.
알레르기 비염 약물 치료에 쓰는 항히스타민제에 관해 말씀을 해주세요.
A.
- 항히스타민제는 비만세포(마스터 세포)와 호염기성 세포에서 나오는 히스타민 고립체가 세포 섭수체에 결합되지 못하게 차단시켜 알레르기성 질환을 치료하는 데 쓰는 약물을 통틀어 항히스타민제라고 합니다.
- 항히스타민제는 1세대 항히스타민제와 2세대 항히스타민제로 나누어집니다.
- 페리액틴(Periactin), 클로트리메톤(Chlor-trimeton), 베나드릴(Benadryl), 피비지(Pyribenzamine) 등의 항히스타민제는 1세대 항히스타민제입니다.
- 1세대 항히스타민제 중 단 한 종류를 선택해 알레르기 비염을 치료할 수 있습니다.
- 1세대 항히스타민제로 치료할 때 알레르기 비염의 치료 효과도 있고 진정제, 수면제 효과도 있어 졸린 증상 등 여러 가지 부작용이 생길 수 있습니다.
- 그래서 요즘에는 2세대 항히스타민제로 알레르기 비염을 주로 치료할 때가 더 많습니다.
- 클라리틴(Claritin),
- 애스테미졸(Astemizole),
- 세티리진(Cetirizine),
- 페소페나딘(Fexofenadine),
- 로라타딘(Loratadine) 등은 2세대 항히스타민제입니다.
- 2세대 항히스타민제로 알레르기 비염을 치료할 때 치료 효과도 좋고 진정 효과는 적고 졸린 증상 등 부작용이 적게 나타날 수 있습니다.
- 항히스타민제로 알레르기 비염을 치료하면 콧물 나는 증상, 재채기하는 증상, 코가 가려운 증상, 눈물 나는 증상은 많이 좋아집니다.
- 비강 점막 충혈완화 효과는 아주 적은 것이 2세대 히스타민 치료제의 단점입니다.
- 그런 이유로, 저녁에 잠자러 들어가기 전에는 1세대 항히스타민제를 복용하고, 낮에는 2세대 항히스타민제로는 치료하는 방법들도 있습니다.
Q.
알레르기 비염 약물 치료에 쓰는 항염증 약물 치료에 관해 말씀을
A.
- 항히스타민제는 히스타민의 작용을 못하게 해서 알레르기 비염을 치료할 수 있습니다.
- 그러나 비강에 생긴 염증은 치료되지 않습니다.
- 그런 염증을 치료하기 위해서 항염증 약물을 사용합니다.
- 항염증 약물에는
- 부데소나이드(Budesonide),
- 플우티카손(Fluticasone),
- 반세나제(Vancenase Aq Nasal Spray 0.084%),
- 베클로메타손(Beclomethasone) 등이 있습니다. 그런 약을 비강 점막에 뿌리는 코르티코스테로이드제 코 분무제로 알레르기 비염을 치료할 수 있습니다
Q.
1세대 항히스타민제로 치료할 때 생기는 부작용은
A.
어떤 종류의 항히스타민제로 치료하든 그 항히스타민제로 알레르기 비염을 치료하는 중 부작용이 생길 수 있고 그 부작용은 항히스타민제의 종류에 따라 다릅니다.
알레르기 비염이나 다른 알레르기 질환을 1세대 항히스타민제로 치료할 때 수면작용, 진정작용, 정신집중이 잘되지 않은 부작용도 있고, 침이 마르는 등의 부작용도 생길 수 있습니다.
그러나 2세대 항히스타민제로 치료할 때는 그런 부작용이 덜 생기는 것이 보통입니다.
Q.
항히스타민제로 치료할 때 한 종류의 항히스타민제로만 치료하나요?
A.
알레르기 비염을 항히스타민제로 치료할 때 한 종류의 항히스타민제로 잘 치료될 수 있지만
때로는 두 종류의 항히스타민제로 동시에 치료해야 치료 효과가 더 잘 나타날 때도 있습니다.
항히스타민제, 비점막층 충혈완화제, 항염증제를 같이 써서 치료할 때도 있습니다.
Q.
한 종류의 항히스타민제로 치료할 때 내성이 생길 수 있나요.
A.
- 있습니다.
- 알레르기 비염의 증상 징후와 정도에 따라 여러 종류의 1세대 항히스타민제 중 1~2 가지를 선택해서 치료할 수 있습니다.
- 1세대 항히스타민제로 알레르기 비염을 치료할 때 치료 시작 후 처음 얼마 동안은 치료효과가 잘 나타나다가 얼마 후에는 치료효과가 더 이상 나타나지 않으면 의사의 지시에 따라 그 1세대 항히스타민제로 더 이상 계속 치료할 필요가 없을 때도 있습니다.
- 한 종류의 항히스타민제로 알레르기 비염을 치료할 때 치료효과가 좋으면 필요에 따라 그 약으로 계속 치료할 수 있습니다.
- 또 한 종류의 항히스타민제로 치료할 때 치료효과가 처음 얼마 동안은 아주 좋았다가 같은 항히스타민제로 장기간 계속 치료하면 치료효과가 점점 떨어질 수 있고 나중에는 아주 치료효과가 없어지는 경우도 있습니다.
- 그래서 다른 종류의 항히스타민제로 바꿔 치료하는 경우도 있습니다.
Q.
알레르기 비염을 항히스타민제로 선택할 때 주의할 점은 무엇이 있나요.
A.
알레르기 비염을 항히스타민제로 치료할 때도 어디까지나 의사의 진단 처방에 따라서 적절한 항히스타민제를 선택해서 치료하는 것이 이상적입니다.
Q.
2세대 항히스타민의 대표적인 것은 무엇이 있나요.
A.
- Loratadine(Claritin), Cetirizine(Zyrtec), Fexofenadine(Allegra),
- and Desloratadine(Clarinex) 등이 있습니다.
- 전에는 의사의 처방이 있어야 이런 2세대 항히스타민제로 치료할 수 있었으나, 요즘엔 Loratadine(Claritin), Cetirizine(Zyrtec) 등 2세대 항히스타민제는 의사의 처방 없이 약국에서 사서 치료할 수 있습니다.
- 2세대 항히스타민제로 알레르기 비염을 치료하면 치료효과도 좋고 잠을 오게 하는 수면부작용도 잘 생기지 않기 때문에 요즘은 1세대 항히스타민으로 치료하지 않는 것이 보통입니다.
Q.
2세대 항히스타민의 부작용은?
A.
진정작용이 덜하고, 졸린 증상 등 부작용이 아주 적게 생깁니다.
2세대 항히스타민제와 비강 점막층 모세혈관충혈 완화제 슈다페드제를 종합해서 만든 알레르기 비염 종합치료 약물도 있습니다.
Q.
슈도에페드린(Pseudoephedrine)제로 알레르기 비염을 치료할 수 있는지요
A.
- 물론입니다.
- 슈다페드제는 알파 아드레날린 작동제입니다.
- 슈다페드로 알레르기 비염을 치료하면 비강 점막층 충혈로 인해 점막층이 부어 코가 막히는 증상이 많이 좋아집니다.
- 이런 종류의 약물들을 비강 점막층 충혈 완화제라고도 합니다.
- 비강 점막층 충혈 완화제는 경구용 알약(정)과 액체 형태로 된 물약이 있고, 비강 속에 분무로 직접 뿌릴 수 있는 분무제도 있고, 또 방울로 비강 속에 떨어트려 넣을 수 있는 비강 점적약제도 있습니다.
- 비강 점막층 충혈완화제의 성분만 들어있는 약물도 있고 항히스타민제와 비강 점막 충혈완화제의 성분을 종합해서 만든 종합 비강 점막층 충혈완화제도 있습니다.
- 요즘 흔히 쓰는 경구용 슈도에페드린은 비강 점막층 충혈완화제의 일종이고, 그 약물 성분 속에는 항히스타민제가 들어 있지 않습니다.
- 그 약물로 치료할 때 항히스타민제의 약리작용은 없고 비강 점막층 충혈완화제 작용만 있습니다.
- 경구용 슈도에퍼드린 등 비강 점막층 충혈완화제는 비강 내 점막층 모세혈관을 일시적으로 강제로 수축시켜서 콧물이 덜 나게 하고 비강 내 점막층 충혈을 일시적으로 가라앉혀 비강 속이 크게 뚫리게 하는 작용이 있습니다.
- 알레르기 비염을 슈다페드제로 치료할 수도 있고, 항히스타민제와 슈다페드제가 든 종합제로 치료할 수 있습니다.
Q.
알레르기 비염을 치료할 때 쓸 수 있는 종합 알레르기 비염 약물도 있나요?
A.
- 물론입니다.
- 1세대 항히스타민제와 알파 아드레날린 작동제를 종합한 약물로 치료할 수 있습니다.
- 페리액틴(Periactin),
- 클로트리메톤(Chlor-trimeton),
- 베나드릴(Benadryl),
- 피비지(Pyribenzamine) 등은 1세대 항히스타민제이고 그중 단 한 가지 1세대 항히스타민제를 선택해 알레르기 비염을 치료할 수도 있고, 1세대 항히스타민제와 비강 점막층 충혈완화제가 든
- 론덱(Rondec),
- 액티페드(Actifed),
- 날데칸(Naldecon),
- 노바페드(Novafed),
- 트리아미닉(Triaminic),
- 다이메탭(Dimetapp) 등 알레르기 비염 치료용 종합 약물들 중 한 종류를 선택해 알레르기 비염을 치료할 수 있습니다.
- 이와 같이 알레르기 비염을 치료하는 데 쓰는 ‘알레르기 약’ 속에는 단 한 종류의 항히스타민제가 들어 있을 수 있고, 항히스타민제와 비강 점막층 충혈완화제도 함께 들어 있을 수 있습니다.
Q.
알레르기 비염을 치료할 때 쓰는 알레르기 비염 치료 종합 약물로 감기를 치료할 수 있나요?
A.
- 물론입니다.
- 감기를 앓을 때 감기의 증상 징후를 경감시켜는 치료에도 이런 종류의 알레르기 비염 치료제로 감기의 증상 징후를 치료하기도 합니다.
- 주의할 것은 이런 약으로 알레르기 비염이나 감기를 치료할 때도 의사의 처방에 따라 치료해야 합니다.
- 특히 4세 이하 영유아들은 이런 종류의 알레르기 비염 치료약인 종합 알레르기 비염 약물로 감기 치료를 해서는 안 됩니다.
Q.
알레르기 비염을 치료할 때 쓰는 비강 속에 직접 넣는 비강 점막층 충혈완화제에 관해서
A.
- 비강 속에 직접 넣는 비강 점막층 충혈완화제로 치료할 수 있습니다.
- 에이프린(Afrin/oxymetazoline)제 코 분무나 네오시네프린(Neosynephrine)제 코 분무는 비강 점막층 충혈을 완화시키는 작용이 있습니다.
- 코 방울약(비 점적약제)을 비강 속에 떨어트려 넣거나 분무를 비강 속에 뿜어 비강 점막층 충혈을 완화시켜 알레르기 비염으로 막힌 비강 속을 속히 뚫어줄 수 있습니다.
- 네오시네프린제에는 코 분무제도 있고, 코 점적약제도 있습니다.
- 에이프린제에는 코 분무제도 있습니다.
- 코 방울약을 비강 점막에 직접 떨어트려 치료하거나 코 분무제로 치료하면 비강 내 점막 충혈이 빨리 일시적으로 경감될 수 있습니다.
- 약의 종류에 따라 비강 점막층 충혈완화의 효과가 6∼12시간 지속될 수 있고, 알레르기 비염으로 막힌 코의 증상이 임시로 좋아질 수 있습니다.
- 이런 약으로 5일 이상 계속 치료하면 비강 점막이 손상될 수 있습니다. 그러므로
- 에이프린제 코 분무나 네오시네프린제 코 분무 등 비강 점막층 충혈 완화제로 치료할 때도 꼭 의사의 처방에 따라서 써야 합니다.
- 이런 약물은 의사의 처방 없이 약국에서 살 수 있습니다.
Q.
알레르기 비염을 치료할 때 쓰는 비만세포 안정제는 어떤 약입니까
A.
- 비만세포 안정제를 비강 속에 직접 뿌려 비만세포 속에 있는 히스타민 과립체가 방출되는 것을 막는 작용이 있습니다.
- 크로몰린(Cromolyn) 코 분무제는 비만세포 안정제이고 비만세포 속 히스타민 과립이 방출되는 것을 막는 약리 작용이 있습니다.
- 기관지 천식이 유발 되지 않게 예방하는데 크로몰린제 코 분무를 씁니다. 크로몰린제 코 분무를 비강 내에 뿌리면 알레르기 비염이 유발되는 것을 예방할 수 있고 이미 생긴 알레르기 비염이 치료될 수 있습니다.
- 크로몰린제 분무를 비강 내에 뿜어 치료하기가 편하고 예방 효과도 좋습니다.
- 크로몰린제 분무를 수 주나 수개월 동안 계속 써도 예방 효과가 계속 좋습니다.
- 크로몰린제 분무의 부작용은 아주 드물게 생깁니다.
- 처방 없이 사서 쓸 수 있으나 값이 비싼 것이 큰 단점입니다.
Q.
알레르기 비염을 치료할 때 쓰는 코르티코스테로이드제에 관해
A.
- 코르티코스테로이드제 분무는 소염제 즉 항염증제입니다.
- 경도의 알레르기 비염은 2세대 항히스타민제를 선택해 우선 치료해 보고 중등도 알레르기 비염이나 중증 알레르기 비염을 치료할 때는 코르티코스테로이드제 코 분무로 우선 선택해 치료해 보는 것이 요즘 경향입니다.
- 베클로메타손(Beclomethasone), 버드손나이드(Budesonide), 트리암시노론(Triamcinolone) 등의 코르티코스테로이드제 코 분무를 비강 속에 직접 뿌려서 알레르기 비염을 치료하기도 합니다.
- 베클로메타손제 코 분무나 버드손나이드제 코 분무는 비강 내에 뿌릴 수 있게 만든 분말 형태 분무와 액체형태 분무, 두 가지가 있습니다.
- 어떤 종류의 코르티코스테로이드제 코 분무는 의사의 처방에 따라 1일 1~2회 양쪽 비강 속에 뿌려 치료합니다.
- 치료의 경과에 따라 몇 주나 몇 달 동안 알레르기 비염을 치료하기도 합니다.
- 일반적으로 비강 내에 뿌리는 코르티코스테로이드제 코 분무로 알레르기 비염을 치료할 때 치료효과는 치료 시작한 후 12시간 경부터 나타나기 시작하는 것이 보통입니다.
- 비 출혈, 안압증가, 녹내장, 신장 성장 지연 등의 부작용이 나타날 수도 있지만, 몇 주 동안 계속 치료해도 그런 부작용이 거의 생기지 않는 것이 보통입니다.
- 특히 코르티코스테로이드제 코 분무로 알레르기 비염을 치료할 때도 의사의 처방에 따라서 그 약을 꼭 써야 합니다.
Q.
코르티코스테로이드제 주사로 알레르기 비염을 치료할 수 있나요
A.
극심한 알레르기 비염이 다른 종류의 치료 방법으로 치료되지 않을 때는 경구용 코르티코스테로이드제나 근육용 Depot corticosteroid제로 며칠 동안 치료할 수 있습니다.
Q.
류코트리엔 수용체 길항제로 치료할 수 있나요?
A.
류코트리엔 수용체 길항제 (Leukotriene-receptor antagonists)로 치료할 수 있습니다.
코 Montelukast sodium (Singulair)으로 치료하면 알레르기 비염의 증상이 확실히 좋아질 수 있습니다.
요즘 류코트리엔 수용체 길항제로 치료하면 자살을 기도하는 경향이 있어 연구 조사하는 중입니다.
Q.
항콜린 작용제( Anticholinergics)로 치료하나요?
A.
항콜린 작용제(Anticholinergics)로 치료할 수 있습니다.
Ipratropium bromide (Nasal Atrovent 0.03%)제 코 분무를 비강 속에 뿌려 알레르기 비염을 치료할 수 있습니다.
맑은 콧물이 많이 날 때 이 종류의 약물로 치료하면 치료 효과가 좋습니다.
Q.
항히스타민제와 코(비) 코르티코스테로이드제로 동시 치료할 수 있나요
A.
할 수 있습니다.
항히스타민제와 코르티코스테로이드제로 동시에 치료할 수 있습니다.
경구용 항히스타민제로 치료가 잘되지 않거나 코르티코스테로이드제 코 분무로 치료가 잘되지 않는 심한 알레르기 비염을 경구용 항히스타민제와 코르티코스테로이드제 코 분무로 동시 치료하면 치료 효과가 아주 좋을 수 있습니다.
Q.
어떤 경우에 항원 면역 요법으로 치료할 수 있나요
A.
적절히 치료해도 잘 치료되지 않은 중등도 알레르기 비염이나 중증 알레르기 비염
전신 코르티코스테로이드제의 치료를 요하는 심한 알레르기 비염
적절한 코르티코스테로이드제로 적절히 치료해도 치료되지 않는 심한 알레르기 비염
부비동염 및, 또는 기관지 천식과 알레르기 비염이 동시에 있을 때는 알레르기 비염을 항원 면역 요법으로 치료할 수 있습니다.
Q.
항원 면역 요법에 관해 설명해 주세요.
A.
- 알레르기 비염을 유발시킬 수 있는 고양이 털이나 개의 털이나 비듬, 초목의 꽃가루, 또는 집안 먼지 진드기 등에서 순수한 항원물질을 정제 추출할 수 있습니다.
- 이렇게 정제 추출된 여러 종류의 항원물질을 알레르기 비염이나 다른 알레르기 질환이 있는 아이들의 피부 표면층에 접촉시키거나 피부층 속에 주입할 때 나타나는 피부 반응의 정도를 보고 그 아이가 가지고 있는 알레르기 질환이 어떤 종류의 항원으로 인해서 유발되는지 알아볼 수 있습니다.
- 알레르기 비염이 있는 아이들에게 시험한 피부반응 검사의 결과에서 알아낸 항원 물질의 극소량을 피하주사로 항원 면역 요법 치료를 할 수 있습니다.
- 처음에는 최소 극소량 항원 물질로 면역 요법을 시작해서 점점 그 용량을 항원 면역 요법 유지용량까지 증가시킨다.
- 항원 면역 요법 유지용량까지 증가시킨 후부터는 그 유지용량을 2~6주 간격으로 주어 항원 면역치료를 하는 것이 보통입니다.
- 이런 항원 면역 요법으로 치료하면 알레르기 비염의 증상이 ⅔ 정도가 경감된다고 합니다. 이와 같이 항원으로 알레르기 비염이 더 이상 생기지 않게 치료하는 법을 항원 면역 요법이라고 한다.
- 항원 면역 요법은 이론적으로 이상적 알레르기 비염 치료법인 것 같지만 알레르기 비염을 치료할 때 여러 가지 이유로 최초 선택 치료 방법은 아닙니다.
- 전에 설명한 바와 같이, 알레젠(항원)을 피하거나 제거, 알레르기 치료약물 치료 및, 또는 항원 제거 및 피함 등으로 적절히 치료해도 알레르기 비염의 증상 징후가 잘 치료되지 않거나 증상 징후가 심해져서 잠을 잘 수도 없고 학교나 집에서 공부하는데 지장도 생기고 일상생활에 지장이 많이 생길 때는 알레르기 비염을 항원 면역 요법으로 치료하는 것이 보통입니다.
- 3세 이전 영유아들의 알레르기 비염은 항원 면역 요법으로 치료되지 않는 것이 일반적입니다.
- 항원 면역 요법으로 알레르기 비염 치료를 받은 4~14세 연령층에 속하는 아이들에게 기관지 천식이 훨씬 덜 생긴다는 연구 결과도 있습니다.
- 항원 면역 요법으로 치료할 때 전신 부작용이 5~10% 정도 생길 수 있고 어떤 부작용은 생명을 위협할 수 있습니다.
- 또 치료비도 상당한 것이 단점입니다.
- 항원 면역 요법을 피하주사로 하는 것이 보통이지만, 서구에서는 혓바닥 밑에 항원을 넣어 항원 면역 요법을 하기도 합니다.
Q.
코르티코스테로이드제와 2세대 항히스타민제로 치료한 결과는
A.
심한 알레르기 비염은 비강 속에 뿌려 쓰는 코르티코스테로이드 코 분무제와 비 진정효과가 아주 적은 2세대 항히스타민제로 치료하면 치료 효과가 아주 좋습니다.
계절성 알레르기 비염의 36~80% 또는 통년성 알레르기 비염의 55~86%는 잘 치료됩니다.
Q.
코브레이션 비갑개 경감치료(Coblation turbinate reduction treatment)란 무슨 치료입니까
A.
만성 알레르기 비염으로 비강 점막층이 충혈되고 비강이 붓고 막힐 수 있습니다.
알레르기 비염이나 다른 원인으로 비갑개가 자극받아 염증이 생기고 비갑개 부피가 커질 수 있습니다. 비강 점막층 조직 손상을 입히지 않고, 붓고 염증이 생기고 커진 비갑개 부피를 감소시키는 외과적 치료방법을 코브레이션 비갑개 경감치료라고 합니다.
코가 막혀(비강 기도 부분이 막혀) 모든 내과적 치료를 다 해도 확연한 치료효과가 없을 때 이 외과적 치료 방법으로 치료해볼 수 있다(출처-Pediatric News, July 2007).
Q.
알레르기 비염이 시작되는 나이는 유발 인자에 따라 다르다고 최근 뉴스에서 들었습니다. 그에 대해 설명을?
A.
- 알레르기 비염이 유발되기 시작되는 나이는 유발 인자에 따라 다릅니다.
- 알레르기 비염으로 고생하는 것도 문제이거니와 그 진료비도 상당합니다.
- 그리고 알레르기 비염을 앓는 아이들에게는 부비동염, 코 폴립, 중이염, 수면 문제, 기관지 천식 등이 생기기 쉽습니다.
- 우유, 달걀, 밀가루 음식, 바퀴벌레, 고양이, 개, 집 먼지 좀 진드기 등이 알레르기 비염을 유발시키는 인자로 ‘잘’ 알려졌습니다.
- 수면장애, 무호흡증, 집중력 결여증, 공부장애, 생산력 감소 등으로 인해 여러 가지 건강문제가 나타날 수 있습니다.
- 알레르기 비염은 1세 이전에도 유발될 수 있지만, 진짜 알레르기 비염은 1세 이전에는 잘 생기지 않습니다.
- 알레르기 비염을 일으키는 데 주 역할을 하는 아이 쥐 이(IgE) 항체는 IgG, IgA, IgM 항체보다 더 늦게 나타나기 때문에 1세 이전에는 알레르기 비염이 잘 생기지 않습니다.
- 화분으로 인해 유발되는 알레르기 비염은 화분에 노출되기 시작한 후 3년 정도 걸리기 때문에 생후 3세 이전에는 화분 알레르기 비염이 생기지 않는 것이 보통입니다.
- 집먼지 진드기로 유발되는 통년성 비염(일 년 내내 증상이 있는 알레르기 비염)은 9세 이전에는 잘 발생되지 않습니다.
- 우유나 우유로 만든 음식물로 인해 유발되는 알레르기 비염은 0.3% 정도입니다.
- 아토피 체질인 아이들에게서 알레르기 비염의 발생률은 그 이상 될 것입니다.
- 알레르기 비염이 있는 생후 2세 이하 유아들의 50%에게 기관지 천식이 발생될 수 있습니다. 그러나 그보다 훨씬 높은 빈도로 발생될 것입니다.
- Fexofenadine(Allegra), Loratadine(Claritin), Cetirizine(Zyrtec) 등은 비 진정 히스타민제이고 이 약으로 치료하는 동안 진정효과가 잘 나타나지 않습니다.
- Azelastine(Astelin)은 항히스타민과 항소염 작용이 있고 비강 내에 뿌려 치료하는 약이다.
- Beclomethasone, Budesonide(RhinocortAqua), Dexamethasone, Flunisolide, Fluticasone propionate, Mometasone furoate, Triamcinolone acetonide 등의 코르티코스테로이드제 코 분무제가 있습니다. 이 코르티코스테로이드제는 항염증 작용이 있습니다. 비강 내 뿌려 알레르기 비염을 치료하는데 쓰는 국소적 알레르기 비염치료제들입니다.
- Atrovent nasal spray는 비점막층 모세혈관 충혈 완화제이고
- Cromolyn sodium제 코 분무는 항염작용(항염증작용)이 있습니다.
- 나이와 알레르기 비염의 주증도에 따라 위에 설명한 약들 중 한 가지나 두 가지 약을 선택해서 알레르기 비염을 치료하면 치료 효과가 대단히 좋습니다.
- 심한 알레르기 비염은 비강 속에 뿌려 쓰는 코르티코스테로이드제 코 분무와 비 진정효과가 아주 적은 2세대 항히스타민제로 치료하면 치료 효과가 아주 좋습니다.
- 계절성 알레르기 비염의 36~80%, 또 통년성 알레르기 비염의 55~86%는 잘 치료됩니다.
- Budesonide제 코 분무에 관한 더 자세한 정보는 www.rhinocortaqua.com)에서 더 얻으시기 바랍니다. 출처 및 참조문헌: Dr. Frederick E. Leickly, Pediatric News, November 2001와 etc.
One hundred Qs & As on allergy rhinitis
Q. Is allergic rhinitis a hereditary disease?
A. That’s right. It is passed down from generation to generation as somatic dominance. The disease can be induced by grandfathers, fathers, sons and daughters in the same household.
Q. Is allergic rhinitis a common disease?
A. • 15-22% of people of all ages in the United States suffer from allergic rhinitis.
• Another study found that 8.8 to 16 percent of Americans suffer from allergic rhinitis.
• According to another study, 20-30% of children and adolescents suffer from allergic rhinitis.
• Its incidence is on the rise.
• 10% of pre-pubertal American children;
• Twenty percent of adolescent children and young adults in the United States have allergic rhinitis.
• According to the results of a survey of 13,579 American children aged 0-17 years, the incidence of allergic rhinitis was 4.8% in the 0-4-year-old group;
• 10.5% of 5-11-year-olds;
• 14.2% of the 12-17-year-olds.
• It is thought that about 10-20 out of 100 children and adolescents have allergic rhinitis. • Allergic rhinitis is the most common chronic disease of the respiratory system.
Figure 3. Allergens that can cause allergic diseases
• Pet hair such as dogs and cats, dander, house dust mites (house dust mites), mold, mold, pollen, drugs, fish or shellfish, milk and milk food, eggs, flour food and cosmetics, chocolate, nuts, peanuts , beans, etc.
• Allergens that are relatively more likely to trigger allergies.
• Children with severe allergic rhinitis may develop adenoid facial features (allergic facial features). Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Q. What are the causes and pathogenesis of allergic rhinitis?
A. As already mentioned, you are born with a genetic factor that is inherited as a body chromosome dominance that can cause allergic rhinitis. In addition, antigens that can cause allergies enter the body through the nose, oral cavity, mucous membranes of the gastrointestinal tract, through the skin or mucous membranes, and through other organs in the body, so that antigen-antibody adverse reactions occur in the nasal mucosa. At that time, histamine granules are released from the mast cells, and other biochemicals work together to cause allergic rhinitis.
Q. What are the antigens that cause allergic rhinitis?
A. • Plant pollen, mold, mold, dog, cat, cow, horse, chicken, and bird hair or dander, feathers, saliva, dead insect powder, house dust mites, house dust can cause allergic rhinitis.
• Allergens such as milk, eggs, chocolate, wheat flour, soybeans, fish and peanuts ingested orally and through the gastrointestinal tract can enter the blood and then reach the mucous membrane of the nasal passages and cause allergic rhinitis.
• Allergens that enter the body through the skin or the mucous membrane of each organ can cause allergic rhinitis.
• Allergic rhinitis can develop in the mucous membranes of the nasal passages when cat hair, dander, or saliva is inhaled directly into the nasal passages.
Picture 5. The food you see in the picture is easy to cause various allergic diseases. Foods such as milk, milk foods, fish, wheat and shellfish, and nuts such as eggs, peanuts, and walnuts can cause allergies more often. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
• When the nasal mucosa is no longer in contact with cat hair, dander, or saliva, it is normal for cat hair, dander, or saliva to no longer cause allergic rhinitis.
• When the nasal mucosa layer comes into contact with cat fur, saliva, dander, etc., allergic rhinitis may recur with cat fur antigens.
Q. What is the mechanism of allergic rhinitis?
A. When an antigen that can cause allergic rhinitis arrives at the nasal mucosa, histamine granules are released from mast cells, and the nasal mucosa is swollen, the nasal capillaries are congested, runny nose, itchy eyes, red and itchy eyes, nose It is common to have symptoms such as blockage of the mouth and breathing with the mouth open. If allergic rhinitis persists for a long time, symptoms such as allergic salt, allergic shine, and malocclusion may occur. In severe cases, adenoids may also develop.
Q. What is the annual medical cost of treating allergic rhinitis in the United States?
A. It is estimated that the cost of medical treatment is $450 million per year.
Q. What are the possible signs of symptoms in children with chronic allergic rhinitis?
A. • In addition to several of the main symptoms described above, sometimes • sleep disorders;
• learning disabilities;
• attention deficit disorder (attention deficit disorder) and, or hyperactivity disorder (hyperactivity disorder);
• Adenoid hypertrophy,
• Tonsil hypertrophy,
• enlarged lymph nodes in the anterior neck region;
• adenoid facial,
• obstructive sleep apnea (sleep-blocked apnea);
• Grinding, malocclusion,
• hypertrichosis,
• Palm excess balance;
• Allergic salute;
• Dennie’s lines;
• You may develop symptoms such as nasal polyps.
Q. Are there other conditions that children with allergic rhinitis may be more likely to develop?
A. Sinusitis, bronchial asthma, eye allergy, otitis media, and conjunctivitis may occur simultaneously.
Q. What is atopic constitution?
A. A constitution that is not a typical normal constitution is called atopic constitution or atopic constitution. There seems to be few people who are not atopic these days. Children with atopic constitution are more prone to allergic diseases such as allergic rhinitis, bronchial asthma (asthma), atopic dermatitis, poison ivy contact dermatitis, and urticaria, and children with the atopic constitution are more likely to develop food allergies.
Q. What is the relationship between allergic rhinitis and bronchial asthma?
A. • Allergic rhinitis can develop in 90% of children with a previous history of bronchial asthma (asthma), and bronchial asthma can be cured if the allergic rhinitis is well treated.
• The incidence of bronchial asthma in children with allergic rhinitis is three times higher than that in children without allergic rhinitis.
• Children with allergic rhinitis have a 40% chance of developing bronchial asthma.
• Allergic rhinitis and bronchial asthma are caused by biochemical mediators such as IgE, cytokines, histamine, and leukotriene, and bronchial asthma can be treated with corticosteroids, bronchodilators, anti-leukotene agents, and anti-IgE agents, and allergic rhinitis is bronchial. Allergic rhinitis, which contains medications used to treat asthma, can be treated well.
Q. What is seasonal allergic rhinitis, perennial allergic rhinitis, and mixed allergic rhinitis? A. • When children with allergic rhinitis caused by mold or mold antigens go to a dry place where mold or mold does not grow, it is normal that the mold or mold antigen will no longer cause allergic rhinitis.
• When the children return to a damp area where mold or mold grows, it is common for the mold or mold antigen to re-initiate allergic rhinitis
• Symptoms of mold or mold-induced allergic rhinitis may be exacerbated in temperatures or seasons where mold or mold grows, such as in summer.
• In addition, children suffering from allergic rhinitis due to allergic rhinitis caused by acacia pollen may develop allergic rhinitis every year with acacia pollen in May to June when acacia flowers are in full bloom.
• This seasonal allergic rhinitis is called seasonal allergic rhinitis.
• Allergic rhinitis caused by ragweed pollen antigens can be induced in the autumn when Ragweed grows, and in New England in the United States, allergic rhinitis is induced a lot in spring with maple tree pollen antigens that bloom a lot in spring.
• Collectively, this type of allergic rhinitis is called seasonal allergic rhinitis. • Allergens such as house dust, house dust mites, molds, or mold that you come into contact with almost daily, or foods you eat almost every day are the most likely triggers for allergic rhinitis. • Allergic rhinitis can be induced year-round in children who come into contact with those kinds of antigens year-round.
• This type of allergic rhinitis is called perennial allergic rhinitis. Perennial allergic rhinitis caused by house dust mites (all-year-round symptomatic allergic rhinitis) is less common in children younger than 9 years of age.
• Many children also have seasonal allergic rhinitis and perennial allergic rhinitis.
• This type of allergic rhinitis is called mixed allergic rhinitis.
Q. What is the relationship between cold or stress and the symptoms of allergic rhinitis? A. In general, symptoms of allergic rhinitis can be much worse when you have a viral upper respiratory infection, such as a cold or flu, or when you are under a lot of stress. Also, the symptoms can get worse when you are exposed to more types of antigens.
Q. What are the typical symptoms of acute allergic rhinitis?
A. • It depends on your age, type of antigen, and whether there are any complications
• Typical symptoms of allergic rhinitis include:
• runny nose
• Stuffy, itchy nose
• sneeze and
• Your eyes may be red, itchy, and watery.
• The roof of the mouth may itch
• These symptoms may recur seasonally and
• These symptoms may be temporary and may occur throughout the season.
• The signs of such symptoms may be mild, moderate, or severe.
Q. Is allergic rhinitis possible in newborns and infants?
A. Theoretically, the symptomatic signs of allergic rhinitis can begin in newborns and at any age thereafter. Allergic rhinitis begins to occur, especially in newborns with atopic constitution, when they start taking artificial nutrition containing milk protein. Although infants who are breastfed are less likely to develop allergic rhinitis, depending on what the mother eats, allergic rhinitis may also develop in newborns and in infants.
Q. What is the incidence of allergic rhinitis that can be caused by milk or milk food?
A. The incidence of allergic rhinitis caused by milk or milk-based foods is about 0.3%.
Q. What is the relationship between artificial nutrition and allergic rhinitis eaten by newborns and infants with atopic constitutions?
A. If newborns or infants, especially those with the atopic constitution, eat artificial nutrition containing milk protein, whole milk, or milk food, milk protein may cause allergic rhinitis.
Q. Can allergic rhinitis worsen when exposed to multiple antigens at once?
A. When children with allergic rhinitis to milk food are exposed to house dust mites, they are more likely to develop allergic rhinitis with house dust mite antigen, and allergic rhinitis caused by milk protein and allergic rhinitis caused by house dust mites. can be triggered at the same time.
Q. What does ‘allergic solution’ mean?
A. If you have an itchy nose with allergic rhinitis, there are symptomatic signs of rubbing your nose with your hands in a saluting position, as if raising your hand to rub your nose. These symptoms are called ‘allergy salute’.
Q. What is the relationship between allergic rhinitis and oral breathing?
A. • If your nose is stuffy due to allergic rhinitis, you often breathe through your mouth with your mouth open.
• This breathing is called ‘mouth breathing’ and also called ‘gaping’.
• If you have chronic allergic rhinitis, you tend to breathe with your mouth open in front of people all day and night.
• There are also stupid adults who sometimes say ‘idiot’ to children who suffer so much.
• Newborns and infants with allergic rhinitis often have a stuffy nose, often breathing with their mouth open.
• This symptom is called gaping in English and ‘mouth breathing’ in Korean.
• If allergic rhinitis is not properly treated, these symptoms may continue from newborn to puberty and may continue into adulthood.
Q. What is the relationship between malocclusion and allergic rhinitis?
A. As allergic rhinitis continues for a long time, oral breathing, enlarged adenoids, enlarged tonsils, changes in the structural interrelationships of the mouth and face, and dental problems may occur. And severe malocclusion can occur. There are pros and cons here too. In my experience, there is a close relationship between malocclusion and allergic rhinitis. So, I think the treatment of allergic rhinitis plays an important role in the treatment of malocclusion.
Q. What is the relationship between allergic rhinitis and adenoids?
A. Allergic rhinitis can cause long-term symptoms of open-mouth breathing. There may be abnormalities in the dentition, such as cavities, occlusions, and malocclusions. Interrelationships of anatomical facial structures such as eyes, nose, mouth, face, and gums may change and abnormalities may occur. Therefore, unusual facial features may appear in children with allergic rhinitis. This face is called the adenoid face.
Q. What is the difference between cold and allergic rhinitis?
A. • A cold is a viral infection that occurs in the upper respiratory tract, such as the nose, nasal passages, pharynx, sinuses, adenoids, and tonsils.
• When you catch a cold, it is common to have a low or high fever, sore throat, and body aches.
• The cold usually goes away on its own within 10 days.
• With allergic rhinitis, the mucous membranes in your nasal passages are swollen, red, stuffy, runny nose, sneezing, and you may not be able to breathe through your nose if your nose is blocked, so you may be able to breathe with your mouth open
• I can’t even sleep well.
• Allergic rhinitis is an allergic disease, and when you have allergic rhinitis, there is no fever, no sore throat, no body aches, and it usually lasts more than 2 weeks.
• Cold and allergic rhinitis are different.
• Sometimes these two ailments can coexist.
Q. What is the relationship between allergic rhinitis and adenoids or tonsils?
A. • Adenoids are a type of lymphoid tissue located at the back of the nasal passages and at the top of the pharynx.
• Adenoids function as a defense against infectious diseases by trapping sulfur sources, bacteria, and viruses that enter through the nose and preventing them from entering the body further than the upper respiratory tract.
• It also traps harmful antigens that enter the body through the nostrils and prevents them from entering the body anymore.
• Excessive use of these functions results in anatomical enlargement of the adenoids.
• In about the same way, the palatine tonsils on either side of the mouth will also grow.
• Abnormally enlarged adenoids and tonsils are common, especially in children with allergic rhinitis.
Q. Children with allergic rhinitis also snort and snore more often, why
A. In children with allergic rhinitis, the adenoids and tonsils become abnormally enlarged, the nose becomes blocked, mouth breathing occurs, and changes in the anatomy of the nasal cavity, palate, and dentition occur. As a result, there are many cases of snoring when talking and snoring when sleeping. Allergic rhinitis, especially in school-age children, can lead to frequent nasal congestion and abnormally large adenoids in the back of the nasal passages and tonsils on either side of the mouth. And that’s why I snort better.
Q. It is said that if you have allergic rhinitis, you may have nosebleeds. Why?
A. With allergic rhinitis, the nasal mucosa is swollen, pale, and moist, and the capillaries in that mucous membrane dilate. Sneezing, coughing, minor trauma to the nose, or even lightly rubbing or touching the nose can rupture the enlarged mucosal capillaries, which can make nosebleeds more likely.
Q. Do you cough even with allergic rhinitis?
A. • If you have allergic rhinitis, you may cough intermittently. In particular, when sleeping at night, runny nose flows into the back of the nasal passages and into the nasopharynx, which stimulates the pharynx, which may cause intermittent coughing while sleeping.
• In addition, 30% of children with allergic rhinitis also have bronchial asthma.
• You can cough because of it, sometimes with both allergic rhinitis and bronchial asthma.
• Most children with bronchial asthma have nocturnal bronchial asthma attacks while they sleep at night, so it is common to cough while sleeping.
• You may have this cough for several days.
• These sleep-induced bronchial asthma attacks are called nocturnal bronchial asthma.
• Differential diagnosis of whether children with allergic rhinitis cough at night, coughing due to nocturnal bronchial asthma, allergic rhinitis, or coughing due to two diseases, allergic rhinitis and nocturnal bronchial asthma Sometimes it’s difficult to do.
Q. If I have allergic rhinitis, can I easily get sinusitis (sinusitis)?
A. • That’s right.
• If you have allergic rhinitis, you may be more prone to sinusitis.
• The nasal mucosa and the sinus mucosa are made of the same type of mucosal cells, and the sinuses and nasal passages are interconnected by small natural vents.
• In addition, the mucosal layer of the airway that caused the allergic rhinitis swells and the passageway can often be blocked by allergic rhinitis.
• Blocked natural vents make your sinuses more prone to bacterial infections and more prone to sinus infections.
• There are normally 8 sinuses on both sides of the face, including the frontal sinuses, ethmoid sinuses, sphenoid sinuses, and maxillary sinuses around the nasal cavity.
• The sinuses in and around the nasal passages are normally connected to each other by small vents.
• The mucosal layer in the duct can swell with allergic rhinitis and block the duct, which can lead to sinusitis (sinusitis) and sinus headaches.
• For this reason, most children with allergic rhinitis are more prone to sinusitis.
Q. Does allergic rhinitis cause frequent headaches?
A. When you have allergic rhinitis, the small air ducts that connect your sinuses to your nasal passages are easily blocked, which can often cause a blocked sinus headache (Sinus headache). In addition, sinusitis can cause a headache as a symptom of sinusitis, and tension fatigue syndrome can occur in children with atopic constitution, which can also cause frequent headaches.
Q. Is allergic rhinitis more prone to otitis media?
A. • You can take it better.
• Allergic rhinitis can cause frequent blockage of the eustachian tube in the posterior nasal airway area.
• This can create negative pressure in the middle ear cavity.
• Exudate may accumulate in the middle ear cavity and cause otitis media.
• This can also lead to bacterial infection of the middle ear cavity effusion, resulting in acute otitis media.
• The bulbar canal (ear tube) may swell and block the ear canal frequently, preventing air from passing between the middle ear cavity and the entrance to the tube in the nasopharyngeal airway.
• You may often have acute otitis media or otitis media with effusion. • Sometimes hearing loss can occur.
Q. Is there a difference between a runny nose when I have allergic rhinitis and a runny nose when I have sinusitis?
A. When there is only allergic rhinitis without complications, it is usually a clear runny nose. However, when allergic rhinitis and bacterial sinusitis occur at the same time, it is common to have a runny nose that is yellow or blue and thicker. Sometimes there is no difference in the runny nose.
Q. Do you have a runny nose if you have allergic rhinitis?
A. A runny nose may not come out even when there is only allergic rhinitis, and a runny nose may not come out when there is only sinusitis. Or, even when both diseases are present at the same time, a clear runny nose may come out little by little, and sometimes there may be no runny nose at all.
Q. Does allergic rhinitis cause allergic diseases in the eyes and mouth?
A. It’s very likely to happen. Allergic diseases in the eyes, sinuses, adenoids, tonsils, pharynx, oral cavity, etc. can be triggered at the same time. For example, allergic conjunctivitis may develop. Allergic conjunctivitis can cause symptoms that include frequent redness of the conjunctiva, red, watery eyes, and itchy eyes and frequent rubbing of the eyes. Allergic rhinitis can often result in a geographic tongue.
Q. I’ve been told that some children with allergic rhinitis can choke during sleep, resulting in apnea, and sometimes painful breathing or snoring, and why?
A. The adenoids of children with atopic constitutions are usually much larger and enlarged than the adenoids of children without atopic constitutions. Also, in most cases, the tonsils are also larger. Because of this, the upper airways, or breathing, in children with allergic rhinitis become much narrower. This can cause shortness of breath during sleep, making it difficult to breathe or snort. Sometimes obstructive apnea (obstructive sleep apnea) also develops.
Q. I read that some of the children with allergic rhinitis had enlarged lymph nodes in the neck just below the lower jaw, why is that?
A. It is common for children with allergic rhinitis to have enlarged lymph nodes in the neck area just below the lower jaw. The lymph nodes in the neck just below the lower jaw, adenoids, and tonsils are also a kind of lymphatic tissue, and the lymphatic tissue has an infectious disease defense function that prevents antigens or bacteria from entering the body through the nasal and pharyngeal cavities through the mouth or nasal passages. Because of such a defensive function, the lymph nodes in the tonsils and neck also become excessively large.
Q. Most children with allergic rhinitis develop a habit of gnashing their teeth at night. Why?
A. If you have allergic rhinitis, your eyes and nose, as well as your pharynx and roof of your mouth, may be itchy. There are some doctors who claim that the pharynx or roof of the mouth is itchy while sleeping, and I unconsciously grind the teeth as a way to relieve the itching by teasing the upper and lower jaws. Most children with allergic rhinitis have a habit of gnashing their teeth at night.
Q. If you have allergic rhinitis, what changes can occur in your mouth and face?
A. Children with allergic rhinitis can experience many changes in the interrelationships of the anatomy of the mouth, face, nose, jaw, teeth, gums, etc., because the nose is often clogged and breathing with the mouth open. One of the resulting tooth changes is malocclusion. The second is adenoid facial hair. It has already been mentioned earlier. Many other changes can occur on the face.
Q. It is said that children with allergic rhinitis sometimes have more body hair, but why? A. Antigens enter the body through the oral, nasal, or skin or mucous membranes. More body hair is produced to prevent any further entry of those antigens through the skin into the body. It is almost the same reason that there is more hair in the nostrils.
Q. How is allergic rhinitis diagnosed?
A. It is common to make a diagnosis by integrating the current medical history, past medical history, family history, symptom signs, and examination findings. Depending on the need, the diagnosis is made by several other methods, such as allergen provoking tests, allergic skin tests, and blood tests.
Q. Do children with allergic rhinitis get colds differently from children without allergic rhinitis?
A. Symptoms of allergic rhinitis can be made worse when children with allergic rhinitis have a cold or other types of viral upper respiratory tract infections. And the symptoms of upper respiratory tract infections, such as a cold, can be much more severe.
Q. What are the common complications and co-morbidities of allergic rhinitis?
A. Children with allergic rhinitis may have co-morbidities such as bronchial asthma, sinusitis, otitis media, atopic dermatitis, food allergy, drug allergy, and insect allergy.
Q. What are the signs and symptoms that are very important in diagnosing allergic rhinitis?
A. • The habit of rubbing the nose while raising the nose because it is itchy can cause horizontal skin wrinkles to form on the skin area on the bridge of the nose, where the tibia and cartilage of the nose are connected. Skin wrinkles are called Dennie lines.
• Signs of raising your hand and rubbing your nose are called ‘allergic salutes’ or ‘allergy salutes’.
• The skin color just under the eyelids under both eyes changes to a dark skin color
. • These are called Allergic shiners.
• Allergic shiners may be temporary, or they may persist for several months or longer.
• Shiner refers to a bruise on the face or any part of the body, which is followed by a temporary darkening of the skin color after a bruise.
• When allergic rhinitis persists for a long time, the anatomical interrelationships of the nose, nasal passages, mouth, adenoids, and tonsils are unusually changed.
• The shape of the face can change to look like a fool’s face.
• This face shape is called an adenoid face, or adenoid face.
• Anomalies are of great value in diagnosing allergic rhinitis.
Q. How is allergic rhinitis diagnosed?
A. As already explained, the diagnosis is mainly made by synthesizing the patient’s past and present medical history, family history, symptom signs, and examination findings. Blood tests, allergic skin tests, parenteral tests as needed. Diagnosis is made by examining the nasal cavity with a nasal endoscopy. If there are symptomatic signs of typical allergic rhinitis, the conjunctiva is congested, and nasal mucosa is pale and abnormally moist when examining the nasal passages, it is very helpful in diagnosing this disease. Other symptoms may include frequent blockage of the ear canal, intermittent coughing, and a feeling of pressure in the sinus area.
Q. Is a family history important in diagnosing allergic rhinitis?
A. A family history of allergic rhinitis such as bronchial asthma, allergic dermatitis, allergic rhinitis, drug allergy, contact dermatitis, or food allergy to one of your biological parents or siblings is very helpful in diagnosing allergic rhinitis. And if any of your biological parents or siblings have atopic constitution, it helps a lot in diagnosing them.
Q. How do you know if allergic rhinitis can also be caused by food allergens?
A. Allergic rhinitis is inherited as somatic chromosomal dominance. Allergic rhinitis can also be caused by food allergens.
A challenge test is one way to find out which foods are causing allergic rhinitis. It can also be diagnosed by avoiding eating those foods.
Q. What is a provocative test
A. • To diagnose allergic rhinitis caused by food allergens, it is also diagnosed with a provocation test.
• Do not eat any food suspected to cause allergic rhinitis for 2 to 4 weeks, and carefully observe whether the symptoms of allergic rhinitis improve, disappear, increase, or change while the food is not eaten for 2 to 4 weeks. do.
• If the symptoms of allergic rhinitis have significantly improved at this time, you can think that the food is most likely causing allergic rhinitis.
• However, it is not possible to make a definitive diagnosis in this way.
• If the symptoms of allergic rhinitis reappear when you then eat the food you suspect was causing the allergic rhinitis, you can think that it is very likely that the food caused the allergic rhinitis.
• This method of diagnosing allergic diseases by identifying the food (antigen) that caused allergic rhinitis in this way is called a challenge test (challenge test).
• Provocation testing should never be done at any time and should never be done at the discretion of the parent or patient.
• Even when allergic rhinitis is mild, your doctor may order a provocative test.
Q. Can I do a provocation test (challenge test) when I suspect that allergic rhinitis is caused by an antigen such as house dust or house dust mites?
A. • You can.
• Children who have had allergic rhinitis caused by antigens such as house dust or house dust mites may show symptoms of allergic rhinitis with itchy nose and sneezing when they are in a house with a lot of house dust or dust mites.
• When these symptoms of allergic rhinitis appear, you may suspect that allergic rhinitis is caused by house dust or house dust mite allergens.
• A skin allergy test usually finds an antigen more often than a challenge test does.
Q. What clinical tests are used to diagnose allergic rhinitis?
A. • IgE blood test;
• nasal mucus test;
• Allergy skin tests;
• blood eosinophil tests;
• Radiation Allergen Absorption Immunoassay (RAST);
• Fiber optic parenteral examination,
• intranasal provocation tests;
• Inspection of air flow in the nasal cavity;
• Nasal endoscopy
• Allergic rhinitis can be diagnosed with a blood flow test in the nasal mucosa.
• In general, it is common to diagnose allergic rhinitis by synthesizing the presence or absence of symptomatic signs of allergic rhinitis, examination findings, etc., without diagnosing with these clinical tests.
Q. Please explain about environmental control treatment and antigen avoidance treatment.
A. • How to avoid or eliminate, as far as possible, all antigens or triggers that can cause allergies.
• Ideal treatment.
• More specifically, it is as follows.
• Allergens that can trigger allergic rhinitis or many other allergic diseases – avoid eating foods as much as possible.
• Allergic rhinitis by breastfeeding or feeding hypoallergenic artificial nutrition to newborns or infants born to siblings of biological parents with allergic diseases or atopic constitution, if possible, instead of feeding artificial nutrition containing milk, milk protein, or soy protein. Prevents this from occurring and properly treats allergic rhinitis that has already occurred.
• To prevent allergic rhinitis and other allergic diseases, you should avoid eating other foods that are likely to trigger allergic diseases as much as possible.
• Foods, especially milk, eggs, and chocolate, are well-known as foods that are more likely to cause allergic rhinitis and other types of allergic diseases.
• Avoid such foods as much as possible. Occasionally, cravings for foods that cause allergic rhinitis may occur, so be careful.
• It is recommended that pets such as dogs, cats and birds be kept out of the house and out of contact if possible.
• Inevitably, when keeping pets in the house, avoid contact with or inhalation of animal fur, saliva, dander, feathers, etc., and bathe the dog frequently.
• Plants and trees should not be raised in the house where children with atopic constitution or allergic rhinitis live.
• Mold and mold grow in damp places such as basements, so adjust the humidity in your home to prevent mold or mold from growing.
• It is better to have a carpet that can be harvested or washed frequently, or not carpeted, as a fixed carpet can collect more house dust and allow dust mites to grow better.
• Curtains should be washed frequently.
• Clean the house from dust and keep dust mites from growing.
• Children with allergic rhinitis or atopic constitution should not place anything other than bedding in the bedroom.
• Cover bed mattresses and spring boxes with plastic covers to keep dust mites from growing.
• In spring, when flowers are in full bloom, close the windows tightly to prevent pollen and mold from entering the house.
• When planting or mowing, pollen or mold can be inhaled into the airways, which can cause allergic rhinitis, allergic conjunctivitis, or bronchial asthma.
• It is difficult to absolutely avoid such antigenic contact, but avoid contact as much as possible.
• Mowing the lawn as needed, wearing a mask and dust-repellent glasses.
• During the regweed flowering season, avoid going to areas where ragweed weeds grow.
• Never wear clothes made from animal or bird feathers, and never use feathers or fur on pillows or blankets
• Reduce house dust mites such as HEPA air filters or Acaricides.
• Get rid of cockroaches.
Q. I would like to know about medication for allergic rhinitis.
A. • Antihistamines There are first-generation antihistamines and second-generation antihistamines.
• anti-inflammatory treatment;
• Antigen Immunotherapy
• Treatment with leukotriene receptor antagonists.
• Treatment with corticosteroids.
• Mast cell (master cell) stabilizer treatment.
• Treatment with nasal mucosal decongestants placed directly into the nasal cavity. • Alpha-adrenergic agonist therapy.
• Comprehensive treatment.
Q. Please tell us about the antihistamines used to treat allergic rhinitis.
A. • Antihistamines Drugs used to treat allergic diseases by blocking the binding of histamine isolates from mast cells (master cells) and basophils to cell receptors are collectively called antihistamines.
• Antihistamines are divided into first-generation antihistamines and second-generation antihistamines.
• Antihistamines such as Periactin, Chlor-trimeton, Benadryl, and Pyribenzamine are first-generation antihistamines.
• Choose only one type of first-generation antihistamine to treat allergic rhinitis.
• When treated with first-generation antihistamines, various side effects such as drowsiness may occur because they have therapeutic effects for allergic rhinitis and have sedative and sedative effects.
• So these days, allergic rhinitis is more often treated with second-generation antihistamines.
• Claritin;
• Astemizole,
• Cetirizine;
• Fexofenadine,
• Loratadine,
etc. are second-generation antihistamines.
• When treating allergic rhinitis with second-generation antihistamines, the treatment effect is good, the sedative effect is small, and side effects such as drowsiness may appear less.
• When allergic rhinitis is treated with antihistamines, the symptoms of runny nose, sneezing, itchy nose, and watery eyes are greatly improved.
• The disadvantage of second-generation histamine therapy is that the nasal mucosa decongestant effect is very small.
• For that reason, there are ways to treat with a first-generation antihistamine before going to bed at night, and with a second-generation antihistamine during the day.
Q. Talk about anti-inflammatory medications used to treat allergic rhinitis
A. • Antihistamines can treat allergic rhinitis by blocking the action of histamine.
• However, inflammation in the nasal passages is not treated.
• Anti-inflammatory drugs are used to treat such inflammation.
• Anti-inflammatory drugs include:
• Budesonide;
• Fluticasone,
• Vancenase (Vancenase Aq Nasal Spray 0.084%),
• Beclomethasone and others. Allergic rhinitis can be treated with a corticosteroid nasal spray, which is sprayed into the nasal mucosa
Q. Side effects of treatment with first-generation antihistamines
A. No matter what type of antihistamine you are treated with, you may experience side effects while treating allergic rhinitis with that antihistamine, and the side effects depend on the type of antihistamine you take. When treating allergic rhinitis or other allergic diseases with first-generation antihistamines, there may be side effects such as sleep, sedation, poor concentration, and side effects such as dry saliva. However, these side effects are less common when treated with second-generation antihistamines.
Q. When treating with an antihistamine, is it only one type of antihistamine?
A. When allergic rhinitis is treated with antihistamines, it can be treated well with one type of antihistamine. Sometimes, treatment with both types of antihistamines is needed to be more effective. It is sometimes treated with antihistamines, nasal decongestants, and anti-inflammatory drugs.
Q. Can tolerance develop when treated with one type of antihistamine?
A. • There is.
• Depending on the symptoms and severity of allergic rhinitis, one or two of several types of first-generation antihistamines can be selected for treatment.
• When treating allergic rhinitis with first-generation antihistamines, if the treatment effect is good for a while for the first time after the start of treatment and the treatment effect is no longer effective after a while, you will no longer need to continue treatment with the first-generation antihistamine according to your doctor Sometimes.
• When treating allergic rhinitis with one type of antihistamine, if the treatment is good, you can continue with that drug as needed.
• In addition, when treated with one type of antihistamine, the therapeutic effect is good for a while, but if you continue treatment with the same antihistamine for a long time, the therapeutic effect may gradually decrease, and then the therapeutic effect may disappear.
• That is why there are cases where treatment is switched to another type of antihistamine.
Q. What should I pay attention to when choosing an antihistamine for allergic rhinitis?
A. Even when treating allergic rhinitis with antihistamines, it is ideal to select and treat the appropriate antihistamine according to the diagnosis and prescription of the doctor.
Q. What are the typical second-generation antihistamines?
A.
• Loratadine (Claritin), Cetirizine (Zyrtec), Fexofenadine (Allegra),
• and Desloratadine (Clarinex).
• Previously, these second-generation antihistamines could be treated with a doctor’s prescription, but these days, second-generation antihistamines such as Loratadine (Claritin) and Cetirizine (Zyrtec) can be purchased from pharmacies and treated without a doctor’s prescription.
• Treatment of allergic rhinitis with second-generation antihistamines is effective in treating allergic rhinitis, and sleep-inducing side effects do not occur.
Q. What are the side effects of second-generation antihistamines?
A. It has less sedation and very few side effects such as drowsiness. There is also a comprehensive treatment drug for allergic rhinitis made by combining the second-generation antihistamine and the nasal mucosal capillary decongestant Sudafed.
Q. Can pseudoephedrine be used to treat allergic rhinitis?
A. • of course
• Sudafed is an alpha-adrenergic agonist.
• If you treat allergic rhinitis with Sudape, the symptoms of nasal congestion due to congestion of the nasal mucosa are greatly improved.
• These types of drugs are also called nasal mucosal decongestants.
• For nasal mucosal decongestants, there are oral tablets (tablets) and liquid potions, sprays that can be sprayed directly into the nasal passages, and nasal drops that can be dropped into the nasal passages as drops.
• Some drugs contain only the components of nasal mucosal decongestants, and there are comprehensive nasal mucosal decongestants made by combining the components of antihistamines and nasal mucosal decongestants.
• Oral pseudoephedrine, which is commonly used these days, is a type of nasal mucosal decongestant and does not contain antihistamines in its components
. • When treated with the drug, there is no pharmacological action of antihistamines, only nasal mucosal decongestant action.
• Nasal mucosal decongestants such as oral pseudoephedrine temporarily forcibly contract the mucosal capillaries in the nasal passages to reduce runny nose and temporarily relieve congestion in the nasal mucosal layers to greatly open the nasal passages.
• Allergic rhinitis can be treated with Sudafed or a combination of antihistamines and Sudafed.
Q. Are there any comprehensive allergic rhinitis medications that can be used to treat allergic rhinitis?
A.
• of course.
• May be treated with a combination of first-generation antihistamines and alpha-adrenergic agonists.
• Periactin,
• Chlor-trimeton;
• Benadryl;
• Pyribenzamine is a first-generation antihistamine, and you can choose only one first-generation antihistamine to treat allergic rhinitis, and it contains a first-generation antihistamine and nasal mucosal decongestant.
• Rondec;
• Activated;
• Naldecon,
• Novafed;
• Triaminic,
• You can treat allergic rhinitis by selecting one of the comprehensive medications for allergic rhinitis, such as Dimetapp.
• In this ‘allergy medicine’ used to treat allergic rhinitis, only one type of antihistamine may be included, and an antihistamine and nasal mucosal decongestant may also be included.
Q. Can a cold be treated with a comprehensive drug for allergic rhinitis used to treat allergic rhinitis?
A.
• of course.
• When you have a cold, this type of allergic rhinitis treatment is sometimes used to treat the symptoms of a cold, even though treatments that relieve the symptoms of the common cold. It is important to note that when treating allergic rhinitis or colds with these drugs, follow the doctor’s prescription
. • Infants, especially children under the age of 4, should not be treated for a cold with this type of allergic rhinitis, comprehensive allergic rhinitis medication.
Q. Regarding the nasal mucosal decongestant that is put directly into the nasal cavity to treat allergic rhinitis
A. • Can be treated with nasal mucosal decongestants that are placed directly into the nasal passages.
• Afrin/oxymetazoline nasal spray or Neosynephrine nasal spray relieves congestion in the nasal mucosa.
• Drop nasal drops (nasal drops) into the nasal passages or spray them into the nasal passages to relieve congestion in the nasal mucosa and quickly clear the nasal passages blocked by allergic rhinitis.
• Neosynephrine includes nasal sprays and nasal drops.
• Aprinze also has a nasal spray.
• Treatment by dropping nasal drops directly onto the nasal mucosa or treatment with nasal sprays can provide quick and temporary relief from mucosal congestion in the nasal passages.
• Depending on the type of drug, the nasal mucosal decongestion effect may last 6 to 12 hours, and the symptoms of blocked nose due to allergic rhinitis may temporarily improve.
• Continued treatment with these drugs for more than 5 days may damage the nasal mucosa. therefore
• When treating with nasal mucosal decongestants such as Aprinze nasal spray or Neosynephrine nasal spray, be sure to follow your doctor’s prescription.
• These drugs can be bought over-the-counter without a doctor’s prescription.
Q. What kind of mast cell stabilizer is used to treat allergic rhinitis?
A. • The mast cell stabilizer is sprayed directly into the nasal cavity to prevent the release of histamine granules in the mast cells.
• Cromolyn nasal spray is a mast cell stabilizer and has a pharmacological action that prevents the release of histamine granules in mast cells.
• Use cromolyn nasal spray to prevent bronchial asthma from triggering. Cromolyn nasal spray can be sprayed into the nasal passages to prevent allergic rhinitis from occurring and to treat pre-existing allergic rhinitis.
- A spray of Cromolyn is sprayed into the nasal cavity for easy treatment and good prevention.
• Continued use of cromolyn spray for weeks or months continues to provide good protection.
• Side effects of Cromolyn spray are very rare.
• It can be purchased without a prescription, but its high cost is a major drawback.
Q. About corticosteroids used to treat allergic rhinitis
A.
• Corticosteroid sprays are anti-inflammatory or anti-inflammatory.
• The current trend is to treat mild allergic rhinitis with a second-generation antihistamine first, and to treat moderate allergic rhinitis or severe allergic rhinitis with corticosteroid nasal spray first.
• Nasal sprays of corticosteroids such as Beclomethasone, Budesonide, and Triamcinolone are sometimes used to treat allergic rhinitis by spraying them directly into the nasal passages.
• Beclomethasone nasal spray and Budesonide nasal spray are available in powder form and liquid form that can be sprayed into the nasal passages.
• Nasal sprays of certain types of corticosteroids are treated by spraying them into both nasal passages 1 to 2 times a day as prescribed by your doctor.
• Depending on the course of treatment, allergic rhinitis may be treated for weeks or months.
• In general, when treating allergic rhinitis with a nasal spray of corticosteroids sprayed into the nasal cavity, the therapeutic effect usually starts to appear about 12 hours after starting treatment.
• Side effects such as nasal bleeding, increased intraocular pressure, glaucoma, and kidney growth retardation may occur, but these side effects are usually negligible after several weeks of treatment.
• Especially when treating allergic rhinitis with corticosteroid nasal spray, you must use the drug according to your doctor’s prescription.
Q. Can corticosteroid injections treat allergic rhinitis?
A. When severe allergic rhinitis is not treated with other types of treatment, it can be treated with oral corticosteroids or intramuscular depot corticosteroids for several days.
Q. Can it be treated with leukotriene receptor antagonists?
A. It can be treated with leukotriene-receptor antagonists. Treatment with nasal Montelukast sodium (Singulair) can definitely improve symptoms of allergic rhinitis. These days, treatment with leukotriene receptor antagonists has a tendency to attempt suicide, which is being investigated.
Q. Is it treated with anticholinergics?
A. It can be treated with anticholinergics. Ipratropium bromide (Nasal Atrovent 0.03%) nasal spray can be injected into the nasal passages to treat allergic rhinitis. When you have a lot of clear runny noses, treatment with this type of drug is effective.
Q. Can antihistamines and nasal corticosteroids be treated at the same time? A. You can. It can be treated simultaneously with antihistamines and corticosteroids.
For severe allergic rhinitis that cannot be treated with oral antihistamines or corticosteroid nasal sprays, simultaneous treatment with oral antihistamines and corticosteroid nasal sprays can be very effective.
Q. In what cases can it be treated with antigen immunotherapy?
A. Moderate or severe allergic rhinitis that is not well treated with adequate treatment Severe allergic rhinitis requiring treatment with systemic corticosteroids Severe allergic rhinitis that cannot be treated with adequate treatment with appropriate corticosteroids Allergic rhinitis can be treated with antigen immunotherapy when sinusitis and or bronchial asthma and allergic rhinitis are coexisting.
Q. Please tell us about antigen immunotherapy.
A.
• Pure antigenic substances can be purified and extracted from cat or dog hair or dander, pollen from plants, or household dust mites, which can cause allergic rhinitis.
• Look at the degree of skin reaction that occurs when the various types of antigen substances extracted in this way are in contact with or injected into the skin layer of children with allergic rhinitis or other allergic diseases, and what type of allergic disease the child has. You can determine if it is caused by an antigen.
• Antigen immunotherapy can be treated by subcutaneously injecting very small amounts of antigenic substances found in skin test results tested in children with allergic rhinitis.
• Start immunotherapy with minimal antigenic substances and gradually increase the dose up to the antigen-immunotherapy maintenance dose.
• Antigen immunotherapy After increasing the maintenance dose, it is normal to administer antigen immunotherapy by giving the maintenance dose every 2 to 6 weeks.
• Treatment with this antigen-immunotherapy reduces the symptoms of allergic rhinitis by one-third. Antigen immunotherapy is a method of treating allergic rhinitis with antigens in this way.
• Antigen immunotherapy, while theoretically an ideal treatment for allergic rhinitis, is not the first choice treatment for allergic rhinitis for a number of reasons.
• As described before, the symptomatic symptoms of allergic rhinitis are not well treated or the symptoms worsened, making it difficult to sleep even when properly treated with avoidance or elimination of allergens, treatment with allergy medications, and elimination and avoidance of allergens. It is common to treat allergic rhinitis with antigen-immunotherapy when studying at school or at home is disrupted or daily life is greatly disrupted.
• Allergic rhinitis in infants and young children before the age of 3 years is not usually treated with antigen-immunotherapy.
• Studies have shown that bronchial asthma is significantly less common in children aged 4 to 14 years who have been treated for allergic rhinitis with antigen-immunotherapy.
• Treatment with antigen-immunotherapy can result in 5 to 10% of systemic side effects, some of which can be life-threatening.
• Another disadvantage is that the cost of treatment is considerable. • Antigen immunotherapy is usually administered by subcutaneous injection, but in the West, antigen immunotherapy is also performed by placing an antigen under the tongue.
Q. Results of treatment with corticosteroids and second-generation antihistamines
A. Severe allergic rhinitis can be treated with a corticosteroid nasal spray and a second-generation antihistamine that has a very little nasal sedative effect, and the treatment effect is very good. 36-80% of seasonal allergic rhinitis or 55-86% of perennial allergic rhinitis are well treated.
Q. What is Coblation turbinate reduction treatment?
A. With chronic allergic rhinitis, the nasal mucosa can become congested and the nasal passages can become swollen and blocked. Allergic rhinitis or other causes can irritate the turbinate, causing it to become inflamed and bulky. A surgical treatment method that reduces the swollen, inflamed and enlarged turbinate volume without damaging the nasal mucosal tissue is called cobration turbinate alleviation therapy. When there is no clear therapeutic effect due to nasal congestion (blockage of the nasal airway) despite all medical treatments, this surgical treatment method can be used (source-Pediatric News, July 2007).
Q.
I’ve heard in the news recently that the age at which allergic rhinitis starts depends on the trigger. explain about him?
A.
• The age at which allergic rhinitis begins depends on the trigger.
• Suffering from allergic rhinitis is also a problem, and the cost of treatment is also high.
• And children with allergic rhinitis are more prone to sinusitis, nasal polyps, otitis media, sleep problems, and bronchial asthma.
• Milk, eggs, flour foods, cockroaches, cats, dogs and house dust mites are “well known” as triggers of allergic rhinitis.
• Various health problems can appear due to sleep disturbance, apnea, lack of concentration, study difficulties, and decreased productivity.
• Allergic rhinitis can develop before 1 year of age, but true allergic rhinitis is less common before 1 year of age.
• Since IgE antibodies, which play a major role in causing allergic rhinitis, appear later than IgG, IgA, and IgM antibodies, allergic rhinitis is less likely to develop before 1 year of age.
• Since pollen-induced allergic rhinitis takes about 3 years after exposure to pollen, it is not common for pollen allergic rhinitis to develop before 3 years of age.
• Perennial rhinitis caused by dust mites (allergic rhinitis with symptoms all year round) is less common before age 9.
• Allergic rhinitis caused by milk or milk-based foods is 0.3%.
• The incidence of allergic rhinitis in children with the atopic constitution will be higher. • Bronchial asthma can develop in 50% of infants under 2 years of age with allergic rhinitis. However, it will occur at a much higher frequency than that.
• Fexofenadine (Allegra), Loratadine (Claritin), and Cetirizine (Zyrtec) are non-sedative histamines and do not have a sedative effect during treatment with this drug.
• Azelastine (Astelin) is a drug that has antihistamine and anti-inflammatory properties and is administered by spraying it into the nasal cavity.
• Corticosteroid nasal sprays such as Beclomethasone, Budesonide (RhinocortAqua), Dexamethasone, Flunisolide, Fluticasone propionate, Mometasone furoate, and Triamcinolone acetonide are available. These corticosteroids have anti-inflammatory properties. These are topical allergic rhinitis medications used to treat allergic rhinitis by spraying intranasally.
• Atrovent nasal spray is a nasal capillary decongestant.
• Cromolyn sodium nasal spray has anti-inflammatory (anti-inflammatory) properties.
• Depending on the age and severity of allergic rhinitis, treatment of allergic rhinitis by selecting one or two of the above-mentioned drugs is very effective.
• Severe allergic rhinitis can be treated with a corticosteroid nasal spray and a second-generation antihistamine with minimal nasal sedative effect, and the treatment effect is very good.
• 36-80% of seasonal allergic rhinitis and 55-86% of perennial allergic rhinitis are cured well.
• For more information on nasal spray with Budesonide, please visit www.rhinocortaqua.com. Sources and references: Dr. Frederick E. Leickly, Pediatric News, November 2001 and etc.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- A SUPPLEMENT TO PEDIATRICS, SYNAPSIS BOOK, BEST ARTICLES RELEVANT TO PEDIATRIC ALLERGY, ASTHMA, IMMUNOLOGY, PEDIATRICS OFFICIAL JOURNAL OF THE AMERICAN ACADEMY.12/2019
- Pediatrics, December 2021-Supplement to pediatrics- best article relate to pediatric allergy , asthma, immunology
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.